Transumbilical Single Port Laparoscopic Adrenalectomy: A Technical Report on Right and Left Adrenalectomy Using the Glove Port
- Affiliations
-
- 1Division of Hepatobiliary and Pancreas, Department of Surgery, Yonsei University College of Medicine, Clinic of Pancreatic and Biliary Cancer, Institute of Gastroenterology, Yonsei University Health System, Seoul, Korea. wjlee@yuhs.ac
- KMID: 1120216
- DOI: http://doi.org/10.3349/ymj.2012.53.2.442
Abstract
- Recently, single port laparoscopic surgery has been the focus of attention due to the advanced laparoscopic skills accumulated from experience and developments in laparoscopic instruments. Herein, we present two cases of initial single port laparoscopic adrenalectomies. Case 1 was a 38-year-old female patient diagnosed with primary hyperaldosteronism because of a the right adrenal 2.5-cm sized adenoma, and case 2 was a 31-year-old female patient diagnosed with primary adrenal Cushing's syndrome because of a left adrenal 2.9-cm sized adenoma. Both patients successfully underwent single port laparoscopic adrenalectomies via a transumbilical transperitoneal approach. There was no estimated blood loss and the total operating times were 60 and 70 minutes, respectively. Both patients recovered uneventfully. We believe that this technique presented could provide potential benefits (lesser wound pain, better cosmetic satisfaction, and shorter convalescence) if the indications are carefully selected.
Keyword
MeSH Terms
Figure
-
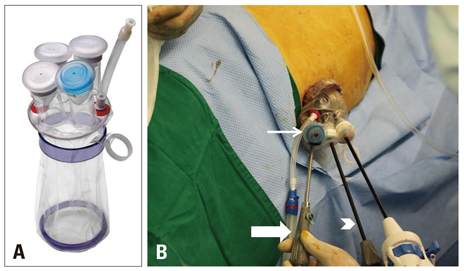
Fig. 1 Glove port and external view of instruments of the case 1. (A) The Glove port is composed of two rings and four trocar channels with gas insufflation and exsufflation lines. (B) The laparoscope camera is inserted through the blue trocar channel (thin arrow), which should be placed in the 6-o'clock position. The articulating hook coagulator and long shaft grasper (arrow head) are working instruments and the snake retractor (thick arrow) is applied for liver retraction.
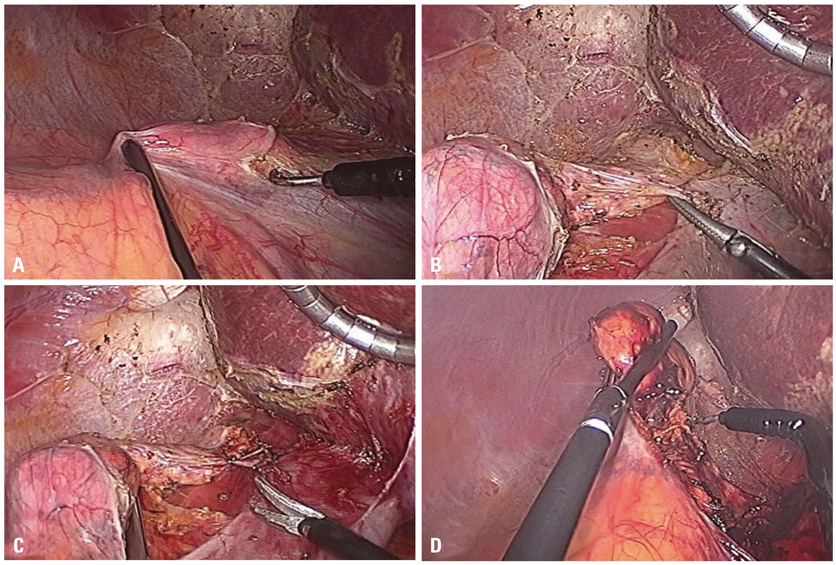
Fig. 2 Operative findings of case 1. (A) The retroperitoneum covering the adrenal gland and inferior vena cava was incised using the articulating hook coagulator with an aid of a long straight laparoscopic grasper. (B) The adrenal vein was carefully isolated using the articulating dissector. (C) The adrenal vein was ligated using 5 mm endo-clips and resected. (D) The tissues around the adrenal gland were completely dissected using the articulating hook coagulator with clipping of vasculatures.

Fig. 3 Postoperative wound of the patient in case 1.
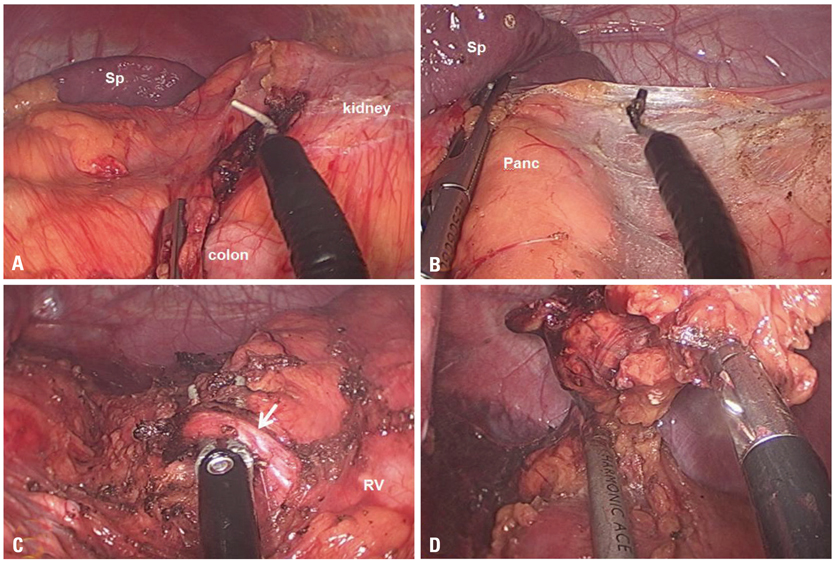
Fig. 4 Operative findings of case 2. (A) The white line of Toldt was dissected using an articulating laparoscopic hook coagulator with an aid of the laparoscopic grasper. (B) The lienorenal ligament was incised, and the dissection was deepened through the plane between the colonic mesentery and Gerota's fascia retracting the pancreas and spleen medially with the laparoscopic grasper. (C) The left adrenal vein (arrow) was identified and isolated. (D) The tissues around the adrenal gland were completely dissected using the harmonic scalpel. Sp, spleen; Panc, pancreas; RV, renal vein.
Cited by 1 articles
-
Single-incision laparoscopic cholecystectomy using instrumental alignment in robotic single-site cholecystectomy
Sung Yub Jeong, Jin Woo Lee, Sung Hoon Choi, Sung Won Kwon
Ann Surg Treat Res. 2018;94(6):291-297. doi: 10.4174/astr.2018.94.6.291.
Reference
-
1. Jacobs JK, Goldstein RE, Geer RJ. Laparoscopic adrenalectomy. A new standard of care. Ann Surg. 1997. 225:495–501.2. McKinlay R, Mastrangelo MJ Jr, Park AE. Laparoscopic adrenalectomy: indications and technique. Curr Surg. 2003. 60:145–149.
Article3. Gagner M, Pomp A, Heniford BT, Pharand D, Lacroix A. Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures. Ann Surg. 1997. 226:238–246.4. Smith CD, Weber CJ, Amerson JR. Laparoscopic adrenalectomy: new gold standard. World J Surg. 1999. 23:389–396.
Article5. Walz MK, Alesina PF. Single access retroperitoneoscopic adrenalectomy (SARA)--one step beyond in endocrine surgery. Langenbecks Arch Surg. 2009. 394:447–450.
Article6. Castellucci SA, Curcillo PG, Ginsberg PC, Saba SC, Jaffe JS, Harmon JD. Single port access adrenalectomy. J Endourol. 2008. 22:1573–1576.
Article7. Chung SD, Huang CY, Wang SM, Tai HC, Tsai YC, Chueh SC. Laparoendoscopic single-site (LESS) retroperitoneal adrenalectomy using a homemade single-access platform and standard laparoscopic instruments. Surg Endosc. 2011. 25:1251–1256.
Article8. Cindolo L, Gidaro S, Neri F, Tamburro FR, Schips L. Assessing feasibility and safety of laparoendoscopic single-site surgery adrenalectomy: initial experience. J Endourol. 2010. 24:977–980.
Article9. Jeong BC, Park YH, Han DH, Kim HH. Laparoendoscopic single-site and conventional laparoscopic adrenalectomy: a matched case-control study. J Endourol. 2009. 23:1957–1960.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single port transumbilical total laparoscopic hysterectomy (TLH): initial experience in Korea
- Transumbilical single port total laparoscopic hysterectomy
- Transumbilical Laparoscopic Cholecystectomy with Additional Port: A Single Surgeon's Experience with 291 Cases
- A new glove port for single incision procedure
- A Case of Single Port Laparoscopic Appendectomy and Cholecystectomy in a Fresh Cadaver: A Feasible Procedure
