Topical and Oral Voriconazole in the Treatment of Fungal Keratitis
- Affiliations
-
- 1Department of Ophthalmology, College of Medicine, Kosin University, Busan, Korea. Shdkim@ns.kosinmed.or.kr
- KMID: 1115652
- DOI: http://doi.org/10.3341/kjo.2009.23.1.46
Abstract
- We describe two patients with fungal keratitis refractory to standard antifungal therapy whose conditions were managed with voriconazole. The first case is a patient with endophthalmitis and corneal ulcer due to Candida parapsilosis after receiving a corneal transplant. The patient was treated with amphotericin but showed no signs of improvement. Topical voriconazole, oral voriconazole, and intravitreal voriconazole yielded signs of improvement. The second case is a 63-year-old male who underwent a month of empiric treatment with 0.2% topical amphotericin for fungal keratitis but showed no signs of improvement. Treatment was then provided with 1% voriconazole. Both cases showed effective treatment with voriconazole. Voriconazole may be considered as a new method to treat fungal keratitis refractory to standard antifungal therapy.
Keyword
MeSH Terms
-
Administration, Oral
Antifungal Agents/*administration & dosage
Candidiasis/diagnosis/*drug therapy/microbiology
Cornea/microbiology/pathology
Diagnosis, Differential
Dose-Response Relationship, Drug
Eye Infections, Fungal/diagnosis/*drug therapy/microbiology
Follow-Up Studies
Humans
Keratitis/diagnosis/*drug therapy/microbiology
Male
Middle Aged
Ophthalmic Solutions
Pyrimidines/*administration & dosage
Triazoles/*administration & dosage
Figure
-
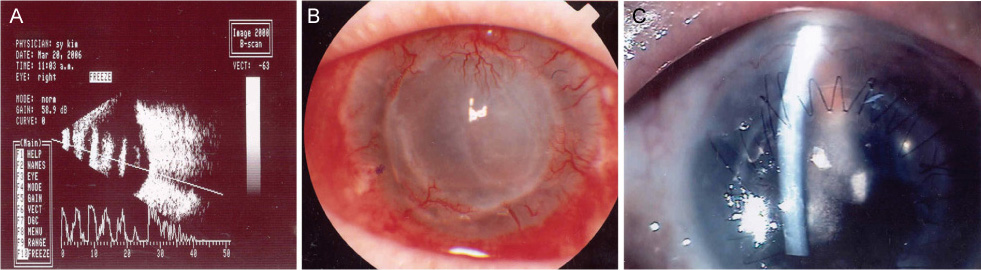
Fig. 1 (A) Approximately 1 year later, anterior chamber hypopyon and vitreous opacity on B-scan were observed. (B) After the patient was treated with 1% topical voriconazole for 6 weeks the corneal lesion and endophthalmitis improved. The corneal opacity persisted as a complication of the lesion and endophthalmitis. (C) The patient underwent another penetrating keratoplasty and showed a visual acuity of 0.1 at follow-up. There was no sign of recurrence.
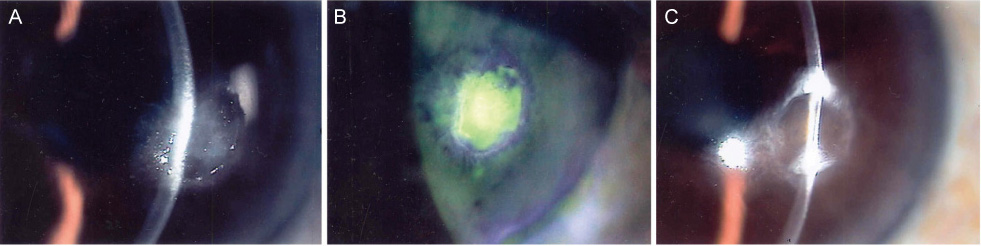
Fig. 2 (A) On initial examination, a feathered corneal infiltration and a corneal ulcer were observed. (B) After 10 days the corneal epithelial appeared healed; however, there was no change in the corneal infiltration. (C) After 13 weeks we observed complete healing of the corneal epithelium and resolution of the corneal infiltrate; however, the corneal opacity persisted.
Cited by 2 articles
-
A Case of Endophthalmitis Treated with Surgical Removal of the Inflammatory Plaque on Corneal Endothelium
Nam Kyun Koo, Kwang Soo Kim, Yu Cheol Kim
J Korean Ophthalmol Soc. 2011;52(8):990-993. doi: 10.3341/jkos.2011.52.8.990.Clinical Effects of Intracameral Voriconazole Injection in Patients with Fungal Keratitis Refractory to Conventional Treatment
Se Hyeong Jeong, Hyo Seok Lee, Jae Kap Cho, Kyung Chul Yoon
J Korean Ophthalmol Soc. 2013;54(5):696-703. doi: 10.3341/jkos.2013.54.5.696.
Reference
-
1. Anderson KL, Mitra S, Salouti R, et al. Fungal keratitis caused by Paecilomyces lilacinus associated with a retained intracorneal hair. Cornea. 2004. 23:516–521.2. Shah KB, Wu TG, Wilhelmus KR, Jones DB. Activity of voriconazole against corneal isolates of Scedosporium apiospermum. Cornea. 2003. 22:33–36.3. Ozbek Z, Kang S, Sivalingam J, et al. Voriconazole in the management of Alternaria keratitis. Cornea. 2006. 25:242–244.4. Kim KH, Kim MJ, Tehah HW. Management of fungal infection with topical and intracameral voriconazole. J Korean Ophthalmol Soc. 2008. 49:1054–1060.5. Jang GJ, Kim KS, Shin WS, Lee WK. Treatment of Candida Chorioretinitis with Voriconazole. Korean J Ophthalmol. 2005. 19:73–76.6. Sponsel W, Chen N, Dang D, et al. Topical voriconazole as a novel treatment for fungal keratitis. Antimicrob Agents Chemother. 2006. 50:262–268.7. Lee SB, Park CJ, Kim JY. A Case of Intravitreal Voriconazole for the Treatment of Drug-resistant Penicillium Endophthalmitis. J Korean Ophthalmol Soc. 2007. 48:1583–1587.8. Haripasad SM, Mieler WF, Holz ER, et al. Determination of vitreous, aqueous, and plasma concentration of orally administered voriconazole in humans. Arch Ophthalmol. 2004. 122:42–47.9. Marangon FB, Miller D, Giaconi JA, Alfonso EC. In vitro investigation of voriconazole susceptibility for keratitis and endophthalmitis fungal pathogens. Am J Ophthalmol. 2004. 137:820–825.10. Gao H, Pennesi M, Shah K, et al. Safety of intravitreal voriconazole: electroretinographic and histopathologic studies. Trans Am Ophthalmol Soc. 2003. 101:183–189.11. Kramer M, Kramer MR, Blau H, et al. Intravitreal voriconazole for the treatment of endogenous Aspergillus endophthalmitis. Ophthalmology. 2006. 113:1184–1186.12. Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002. 347:408–415.13. Miller GR, Rebell G, Magoon RC, et al. Intravitreal antimycotic therapy and cure of mycotic endophthalmitis caused by Paecilomyces lilacinus contaminated pseudophakos. Ophthalmic Surg. 1978. 9:54–63.14. Ozbek Z, Kang S, Sivalingam J, et al. Voriconazole in the management of Alternaria keratitis. Cornea. 2006. 25:242–244.15. Giaconi JA, Marangon FB, Miller D, Alfonso EC. Voriconazole and fungal keratitis: a report of two treatment failures. J Ocul Pharmacol Ther. 2006. 22:437–439.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Fungal Ocular Infection with Topical and Intracameral Voriconazole
- Clinical Efficacy of Topical Voriconazole as Treatment in Culture-Positive Fungal Keratitis
- Clinical Effects of Intracameral Voriconazole Injection in Patients with Fungal Keratitis Refractory to Conventional Treatment
- A Case of Fungal Keratitis Treated with Voriconazole
- A Case of Fungal Keratitis Scedosporium apiospermum
