Polyvinyl Alcohol Embolization Adjuvant to Oily Chemoembolization in Advanced Hepatocellular Carcinoma with Arterioportal Shunts
- Affiliations
-
- 1Department of Radiology, Holy Family Hospital, College of Medicine, The Catholic University of Korea, Kyungki-Do, Korea. hgleehfh@catholic.ac.kr
- 2Department of Radiology, St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 1110728
- DOI: http://doi.org/10.3348/kjr.2007.8.4.311
Abstract
OBJECTIVE
To assess the feasibility and safety of polyvinyl alcohol (PVA) embolization adjuvant to transarterial oily chemoembolization (P-TACE) in advanced hepatocellular carcinoma (HCC) with arterioportal shunts (APS). MATERIALS AND METHODS: Nineteen patients who underwent PVA embolization for APS before a routine chemoembolization (TACE) procedure were retrospectively reviewed. 10 of these 19 patients underwent follow-up TACE or P-TACE after P-TACE (Group A), but nine patients underwent only initial P-TACE because of progression of HCC and/or underlying liver cirrhosis (Group B). Hepatic function tests, APS grades, and portal flow directions were evaluated before and after P-TACE sessions. Complications after procedures and survival days were also evaluated. RESULTS: In group A, APS grade was improved in eight patients and five of six patients with hepatofugal flow showed restored hepatopetal flow postoperatively. No immediate complication was developed in either group. Transient hepatic insufficiency developed in eight (42.1%) of 19 patients after P-TACE, and seven (87.5%) of these eight recovered within two weeks under conservative care. The mean and median survival time all study subjects was 280 days and 162 days. CONCLUSION: P-TACE is feasible and safe in advanced HCC patients with APS.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Antibiotics, Antineoplastic/administration & dosage
Arteriovenous Fistula/therapy
Carcinoma, Hepatocellular/mortality/*therapy
*Chemoembolization, Therapeutic
Contrast Media/administration & dosage
Feasibility Studies
Female
Humans
Iodized Oil/administration & dosage
Liver Circulation
Liver Neoplasms/mortality/*therapy
Male
Middle Aged
Mitomycin/administration & dosage
Polyvinyl Alcohol/*administration & dosage
Retrospective Studies
Treatment Outcome
Figure
-
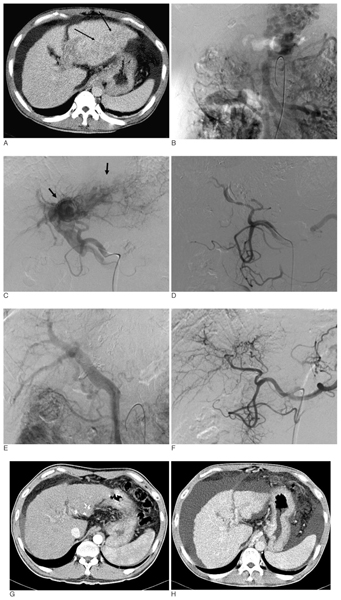
Fig. 1 A 43-year-old male with grade 3 arterioportal shunts and hepatocellular carcinomas (patient 4). A-F. Initial CT (A) revealed a large poorly enhanced mass in the left lobe of a cirrhotic liver and left portal vein thrombosis. Superior mesenteric arterioportogram (B) showing extensive collaterals via the coronary vein and an absent main portal vein. Hepatic arteriogram (C), showing tumor staining and extensive arterioportal shunts (black arrows) in the left hepatic lobe. The main portal vein was opacified by hepatofugal flow. P-TACE (355-500 µm, 1 bottle) was administered to the left hepatic and middle hepatic arteries. Left and middle hepatic arteries were occluded by P-TACE (D). Follow-up superior mesenteric arterioportogram (E) obtained two months after P-TACE, showing restored hepatopetal flow. Hepatic arteriogram (F), showing a non-opacified arterioportal shunts. G, H. Follow-up CT scan (G), six months after P-TACE, showing some lipiodol retention without viable tumor. The tumor and lipiodol retention were not observed by CT (H), 22 months after P-TACE.

Fig. 2 A 51-year-old woman with grade 3 arterioportal shunt and hepatocellular carcinomas (patient 9). On initial hepatic arteriogram (A) showing multiple tumors in both hepatic lobes (black arrows). The main portal vein (white arrow) was opacified indirectly through arterioportal shunt of hepatocellular carcinomas. Polyvinyl alcohol embolization was performed using half a bottle of 355-500 µm sized particles via the right hepatic artery and conventional TACE was performed in both hepatic lobes. Follow-up hepatic arteriogram (B), two months after P-TACE, demonstrating arterioportal shunt improvement. Transarterial chemoembolization was performed without polyvinyl alcohol embolization. After four months, arterioportal shunt recurred in both hepatic lobes with hepatofugal flow in the main portal vein (arrow) on gastroduodenal (C) and right inferior phrenic (D) arteriograms. P-TACE was performed using one bottle of 355-500 µm sized particles into both arteries.
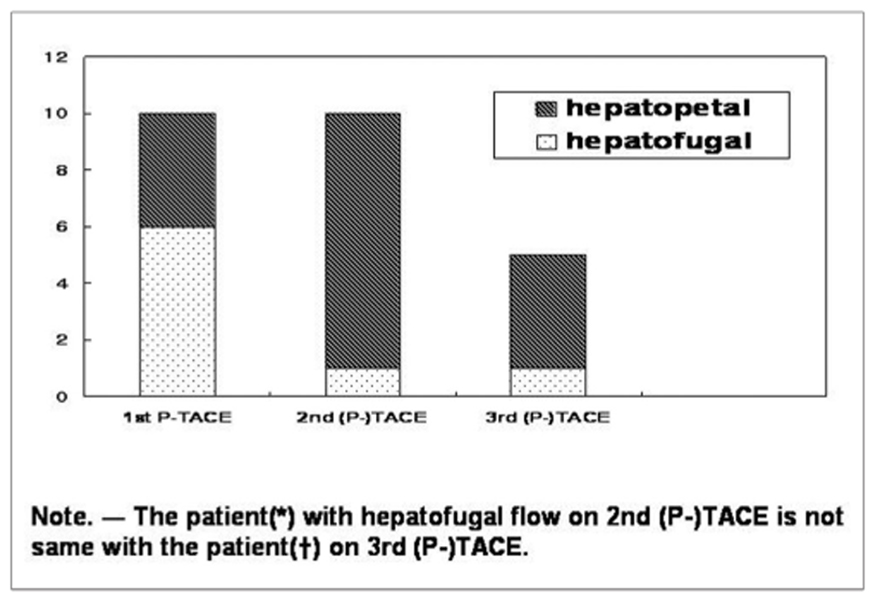
Fig. 3 Number of patients with hepatofugal and hepatopetal flow in group A.

Fig. 4 Cumulative survivals of all study subjects (A) and of the two study groups (B).
Reference
-
1. Ngan H, Peh WC. Arteriovenous shunting in hepatocellular carcinoma: its prevalence and clinical significance. Clin Radiol. 1997. 52:36–40.2. Okuda K, Musha H, Yamasaki T, Jinnouchi S, Nagasaki Y, Kubo Y, et al. Angiographic demonstration of intrahepatic arterioportal anastomoses in hepatocellular carcinoma. Radiology. 1977. 122:53–58.3. Huang MS, Lin Q, Jiang ZB, Zhu KS, Guan SH, Li ZR, et al. Comparison of long-term effects between intra-arterially delivered ethanol and Gelfoam for the treatment of severe arterioportal shunt in patients with hepatocellular carcinoma. World J Gastroenterol. 2004. 10:825–829.4. Yamada R, Sato M, Kawabata M, Nakatsuka H, Nakamura K, Takashima S. Hepatic artery embolization in 120 patients with unresectable hepatoma. Radiology. 1983. 148:397–401.5. Furuse J, Iwasaki M, Yoshino M, Konishi M, Kawano N, Kinoshita T, et al. Hepatocellular carcinoma with portal vein tumor thrombus: embolization of arterioportal shunts. Radiology. 1997. 204:787–790.6. Tarazov PG. Intrahepatic arterioportal fistulae: role of transcatheter embolization. Cardiovasc Intervent Radiol. 1993. 16:368–373.7. Lee DH, Yoon HK, Song HY, Kim GC, Hwang JC, Sung KB. Embolization of severe arterioportal shunts in the patients with hepatocellular carcinoma: safety and influence on patient survival. J Korean Radiol Soc. 1999. 41:1117–1125.8. Coldwell DM, Stokes KR, Yakes WF. Embolotherapy: agents, clinical applications, and techniques. Radiographics. 1994. 14:623–643.9. Siskin GP, Englander M, Stainken BF, Ahn J, Dowling K, Dolen EG. Embolic agents used for uterine fibroid embolization. AJR Am J Roentgenol. 2000. 175:767–773.10. Doppman JL, Girton ME. Bile duct scarring following ethanol embolization of the hepatic artery: an experimental study in monkeys. Radiology. 1984. 152:621–626.11. Bendszus M, Klein R, Burger R, Warmuth-Metz M, Hofmann E, Solymosi L. Efficacy of trisacryl gelatin microspheres versus polyvinyl alcohol particles in the preoperative embolization of meningiomas. AJNR Am J Neuroradiol. 2000. 21:255–261.12. Wachsberg RH, Bahramipour P, Sofocleous CT, Barone A. Hepatofugal flow in the portal venous system: pathophysiology, imaging findings, and diagnostic pitfalls. Radiographics. 2002. 22:123–140.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes in Arterioportal Shunts in Hepatocellular Carcinoma Patients with Portal Vein Thrombosis Who Were Treated with Chemoembolization Followed by Radiotherapy
- Embolization of Seve re Arterioportal Shunts in the Patients with Hepatocellular Carcinoma: Safety and Influence on Patient Survival
- Guidewire-Induced Perforation of Distal Circumflex Artery Treated with Transcatheter Embolization of Polyvinyl Alcohol Form
- Combination treatment with intrahepatic arterial infusion and intratumoral injection chemotherapy in patients with far-advanced hepatocellular carcinoma and arterioportal or arteriovenous shunts: preliminary results
- A Case of Bilateral Uterine Arterial Embolization to Treat Uterine Myoma
