Extraarticular Subtalar Arthrodesis for Pes Planovalgus: An Interim Result of 50 Feet in Patients with Spastic Diplegia
- Affiliations
-
- 1Department of Orthopaedic Surgery, Soonchunhyang University Hospital, Soonchunhyang University College of Medicine, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 3Department of Orthopaedic Surgery, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. pedhkim@yuhs.ac
- KMID: 1110344
- DOI: http://doi.org/10.4055/cios.2010.2.1.13
Abstract
-
BACKGROUND: There are no reports of the pressure changes across the foot after extraarticular subtalar arthrodesis for a planovalgus foot deformity in cerebral palsy. This paper reviews our results of extraarticular subtalar arthrodesis using a cannulated screw and cancellous bone graft.
METHODS
Fifty planovalgus feet in 30 patients with spastic diplegia were included. The mean age at the time of surgery was 9 years, and the mean follow-up period was 3 years. The radiographic, gait, and dynamic foot pressure changes after surgery were investigated.
RESULTS
All patients showed union and no recurrence of the deformity. Correction of the abduction of the forefoot, subluxation of the talonavicular joint, and the hindfoot valgus was confirmed radiographically. However, the calcaneal pitch was not improved significantly after surgery. Peak dorsiflexion of the ankle during the stance phase was increased after surgery, and the peak plantarflexion at push off was decreased. The peak ankle plantar flexion moment and power were also decreased. Postoperative elevation of the medial longitudinal arch was expressed as a decreased relative vertical impulse of the medial midfoot and an increased relative vertical impulse (RVI) of the lateral midfoot. However, the lower than normal RVI of the 1st and 2nd metatarsal head after surgery suggested uncorrected forefoot supination. The anteroposterior and lateral paths of the center of pressure were improved postoperatively.
CONCLUSIONS
Our experience suggests that the index operation reliably corrects the hindfoot valgus in patients with spastic diplegia. Although the operation corrects the plantar flexion of the talus, it does not necessarily correct the plantarflexed calcaneus and forefoot supination. However, these findings are short-term and longer term observations will be needed.
MeSH Terms
-
Adolescent
Arthrodesis/*methods
Bone Screws
Bone Transplantation
Cerebral Palsy/*complications
Child
Child, Preschool
Female
Flatfoot/etiology/radiography/*surgery
Foot/radiography
Foot Deformities, Acquired/etiology/*surgery
Humans
Leg
Male
Muscle Spasticity/complications
Muscle, Skeletal/surgery
Postoperative Complications
Subtalar Joint/radiography/surgery
Walking/physiology
Figure
-

Fig. 1 Foot pressure was measured in 9 areas including the hallux, each metatarsal head, midfoot, and calcaneus. The white curved line represents the path of the center of pressure.

Fig. 2 The pressure-time curves of the foot. If the sole is divided into two regions, shaded areas a and b represent the pressure-time integral of each region. Summation of a and b equals the total impulses. Relative vertical impulse of each region was calculated as a pressure-time integral of that region divided by the total impulses
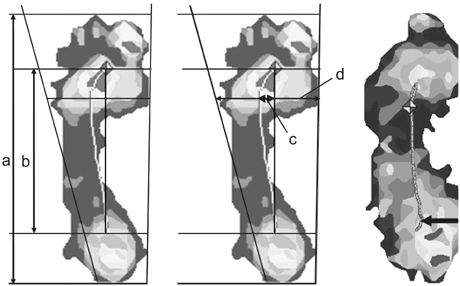
Fig. 3 The path of the center of pressure is represented as a curved white line, and a construction line is drawn from the first to the last center of the pressure data point. The length (a) represents anteroposterior length of the foot; the length (b) anteroposterior length of the path of the center of pressure; the length (c) the lateral deviation of the center of pressure from the construction; the length (d) the maximum width of the foot. Anteroposterior index of the path of the center of pressure (%) = (b / a) × 100. Center of pressure excursion index (%) = (c / d) × 100. The black arrow represents the initial medial deviation of the path of the center of pressure in a patient who underwent an extraarticular subtalar arthrodesis.

Fig. 4 Anteroposterior and lateral radiographs of the foot showing anteroposterior and lateral talocalcaneal angles. Before surgery (A), talonavicular subluxation and plantarflexion of talus was noted. At the final follow up (B), talonavicular subluxation was reduced and plantarflexion of the talus was corrected. However, calcaneal pitch was not corrected accordingly.
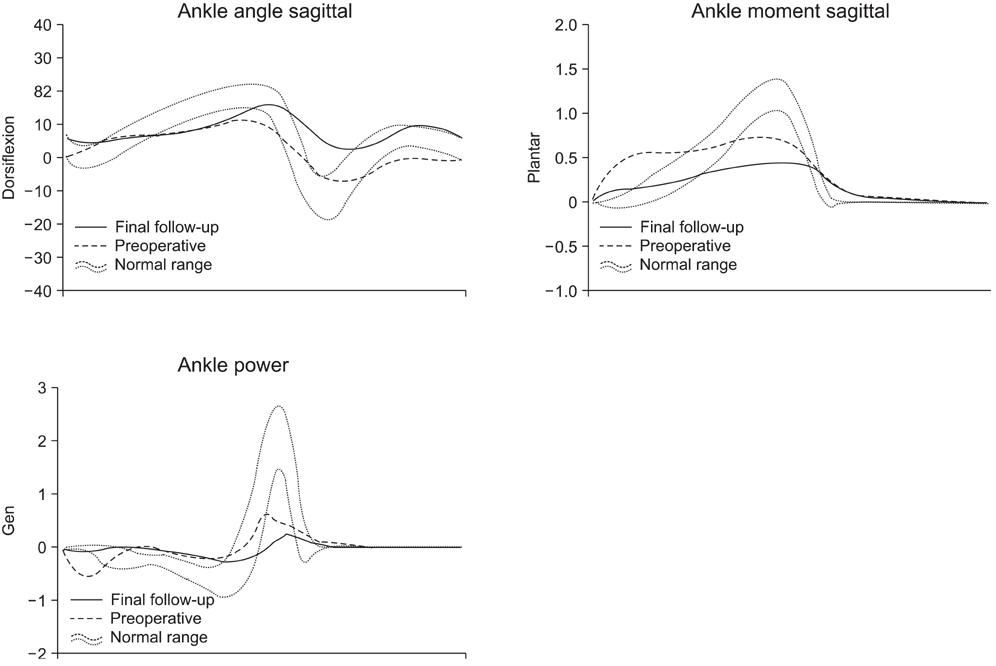
Fig. 5 Sagittal plane kinematic and kinetic changes in the ankle before and after surgery.

Fig. 6 Relative vertical impulse before and after surgery. MT: Metatarsal head, Lat M: Lateral midfoot, Med M: Medial midfoot, Lat C: Lateral calcaneus, Med C: Medial calcaneus.
Reference
-
1. Grice DS. An extra-articular arthrodesis of the subastragalar joint for correction of paralytic flat feet in children. J Bone Joint Surg Am. 1952. 34(4):927–940.
Article2. Alman BA, Craig CL, Zimbler S. Subtalar arthrodesis for stabilization of valgus hindfoot in patients with cerebral palsy. J Pediatr Orthop. 1993. 13(5):634–641.
Article3. Bratberg JJ, Scheer GE. Extra-articular arthrodesis of the subtalar joint: a clinical study and review. Clin Orthop Relat Res. 1977. (126):220–224.4. Jeray KJ, Rentz J, Ferguson RL. Local bone-graft technique for subtalar extraarticular arthrodesis in cerebral palsy. J Pediatr Orthop. 1998. 18(1):75–80.
Article5. Dennyson WG, Fulford GE. Subtalar arthrodesis by cancellous graft s and metallic internal fixation. J Bone Joint Surg Br. 1976. 58(4):507–510.6. Barrasso JA, Wile PB, Gage JR. Extraarticular subtalar arthrodesis with internal fixation. J Pediatr Orthop. 1984. 4(5):555–559.
Article7. Hadley N, Rahm M, Cain TE. Dennyson-Fulford subtalar arthrodesis. J Pediatr Orthop. 1994. 14(3):363–368.8. Sutherland DH, Davids JR. Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res. 1993. (288):139–147.9. Davids JR, Ounpuu S, DeLuca PA, Davis RB 3rd. Optimization of walking ability of children with cerebral palsy. Instr Course Lect. 2004. 53:511–522.
Article10. Rathjen KE, Mubarak SJ. Calcaneal-cuboid-cuneiform osteotomy for the correction of valgus foot deformities in children. J Pediatr Orthop. 1998. 18(6):775–782.
Article11. Herring JA. Herring JA, Tachdjian MO, editors. Disorders of the foot. Tachdjian's pediatric orthopaedics: from the Texas Scottish Rite Hospital for children. 2002. Vol 2:3rd ed. Philadelphia: WB Saunders;891–1037.12. Femery V, Moretto P, Renaut H, Thevenon A, Lensel G. Measurement of plantar pressure distribution in hemiplegic children: changes to adaptive gait patterns in accordance with deficiency. Clin Biomech (Bristol, Avon). 2002. 17(5):406–413.
Article13. Kirtley C. Kirtley C, editor. Plantar pressure measurement. Clinical gait analysis: theory and practice. 2006. Oxford: Churchill Livingstone;97–115.
Article14. Ledoux WR, Hillstrom HJ. The distributed plantar vertical force of neutrally aligned and pes planus feet. Gait Posture. 2002. 15(1):1–9.
Article15. Huber H, Dutoit M. Dynamic foot-pressure measurement in the assessment of operatively treated clubfeet. J Bone Joint Surg Am. 2004. 86(6):1203–1210.
Article16. Mosca VS. Calcaneal lengthening for valgus deformity of the hindfoot: results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am. 1995. 77(4):500–512.
Article17. Bowen TR, Miller F, Castagno P, Richards J, Lipton G. A method of dynamic foot-pressure measurement for the evaluation of pediatric orthopaedic foot deformities. J Pediatr Orthop. 1998. 18(6):789–793.
Article18. Chang CH, Miller F, Schuyler J. Dynamic pedobarograph in evaluation of varus and valgus foot deformities. J Pediatr Orthop. 2002. 22(6):813–818.
Article19. Johnson CH, Christensen JC. Biomechanics of the first ray. Part I. The effects of peroneus longus function: a three-dimensional kinematic study on a cadaver model. J Foot Ankle Surg. 1999. 38(5):313–321.
Article20. Park KB, Park HW, Lee KS, Joo SY, Kim HW. Changes in dynamic foot pressure after surgical treatment of valgus deformity of the hindfoot in cerebral palsy. J Bone Joint Surg Am. 2008. 90(8):1712–1721.
Article21. Bourelle S, Cottalorda J, Gautheron V, Chavrier Y. Extra-articular subtalar arthrodesis: a long-term follow-up in patients with cerebral palsy. J Bone Joint Surg Br. 2004. 86(5):737–742.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatments and Clinical Outcomes for Idiopathic Osteoarthritis of the Tarsometatarsal Joints
- Surgical Treatment for Planovalgus Foot in Children with Generalized Ligamentous Laxity
- Evaluation of the Outcomes according to Etiology in the Pediatric Pes Planovalgus after Lateral Column Lengthening: By Radiologic and Pedobarographic Measurements
- Comparison of Posterior Fixation Technique and Anterior-Posterior Fixation Technique in Subtalar Arthrodesis
- Primary Subtalar Arthrodesis for the Treatment of Intra-articular Calcaneal Comminuted Fractures
