3D Whole-Heart Coronary MR Angiography at 1.5T in Healthy Volunteers: Comparison between Unenhanced SSFP and Gd-Enhanced FLASH Sequences
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Yonsei University Health System, Seoul 135-720, Korea. thkim1@yuhs.ac
- KMID: 1101921
- DOI: http://doi.org/10.3348/kjr.2011.12.6.679
Abstract
OBJECTIVE
To validate the optimal cardiac phase and appropriate acquisition window for three-dimensional (3D) whole-heart coronary magnetic resonance angiography (MRA) with a steady-state free precession (SSFP) sequence, and to compare image quality between SSFP and Gd-enhanced fast low-angle shot (FLASH) MR techniques at 1.5 Tesla (T).
MATERIALS AND METHODS
Thirty healthy volunteers (M:F = 25:5; mean age, 35 years; range, 24-54 years) underwent a coronary MRA at 1.5T. 3D whole-heart coronary MRA with an SSFP was performed at three different times: 1) at end-systole with a narrow (120-msec) acquisition window (ESN), 2) mid-diastole with narrow acquisition (MDN); and 3) mid-diastole with wide (170-msec) acquisition (MDW). All volunteers underwent a contrast enhanced coronary MRA after undergoing an unenhanced 3D true fast imaging with steady-state precession (FISP) MRA three times. A contrast enhanced coronary MRA with FLASH was performed during MDN. Visibility of the coronary artery and image quality were evaluated for 11 segments, as suggested by the American Heart Association. Image quality was scored by a five-point scale (1 = not visible to 5 = excellent). The signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were evaluated at the proximal coronary arteries.
RESULTS
The SSFP sequence rendered higher visibility coronary segments, higher image quality, as well as higher SNR and CNR than the Gd-enhanced FLASH technique at 1.5T (p < 0.05). The visibility of coronary segments, image quality, SNR and CNR in the ESN, MDN and MDW with SSFP sequence did not differ significantly.
CONCLUSION
An SSFP sequence provides an excellent method for the 3D whole-heart coronary MRA at 1.5T. Contrast enhanced coronary MRA using the FLASH sequence does not help improve the visibility of coronary segments, image quality, SNR or CNR on the 3D whole-heart coronary MRA.
Keyword
MeSH Terms
Figure
-

Fig. 1 Schematic diagram of cardiac phase and acquisition window optimization for 3D whole-heart coronary MR angiography with steady-state free precession sequence: end-systole with narrow (120-msec) acquisition window (ESN); mid-diastole with narrow acquisition (MDN); and mid-diastole with wide (170-msec) acquisition window (MDW). Gd-enhanced coronary MR angiography with fast low-angle shot technique was performed in mid-diastole with narrow acquisition condition.

Fig. 2 Volume rendered and curved multiplanar reformatted images of coronary arteries from 3D whole-heart coronary MR angiography at 1.5T. Right and left coronary arteries including posterior descending artery were well-defined on volume rendered (A, B) and curved multiplanar reconstruction (C, D) images obtained at mid-diastole with narrow acquisition. However, right coronary artery and posterior descending artery were blurred on curved multiplanar reformatted image obtained using Gd-enhanced MR angiography at mid-diastole with narrow acquisition, which showed lower signal-to-noise and contrast-to-noise ratios (E).
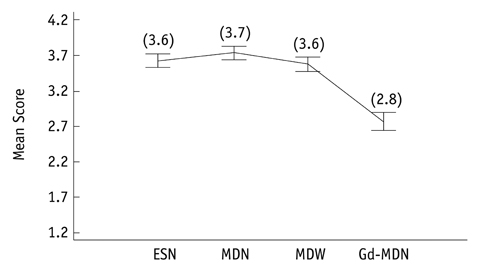
Fig. 3 Graph represents mean image quality scores for coronary artery segments based on five-point scale: 1, not visible; 2, poor; 3, fair; 4, good; and 5, excellent. Images obtained at end-systole with narrow acquisition (ESN), mid-diastole with narrow acquisition (MDN), and mid-diastole with wide acquisition (MDW) did not differ significantly in quality. Gd-enhanced MR angiography at mid-diastole with narrow acquisition (Gd-MDN) produced coronary artery images significantly lower in quality than those obtained by other three methods with steady-state free precession (p < 0.01). Numbers in parenthesis were mean image scores.
Cited by 1 articles
-
Optimizing the Imaging Protocol for
Ex Vivo Coronary Artery Wall Using High-Resolution MRI: An Experimental Study on Porcine and Human
Jiong Yang, Tao Li, Xiaoming Cui, Weihua Zhou, Xin Li, Xinwu Zhang
Korean J Radiol. 2013;14(4):581-588. doi: 10.3348/kjr.2013.14.4.581.
Reference
-
1. Manning WJ, Li W, Edelman RR. A preliminary report comparing magnetic resonance coronary angiography with conventional angiography. N Engl J Med. 1993. 328:828–832.2. Weber OM, Martin AJ, Higgins CB. Whole-heart steady-state free precession coronary artery magnetic resonance angiography. Magn Reson Med. 2003. 50:1223–1228.3. Botnar RM, Stuber M, Danias PG, Kissinger KV, Manning WJ. Improved coronary artery definition with T2-weighted, free-breathing, three-dimensional coronary MRA. Circulation. 1999. 99:3139–3148.4. Johnson KR, Patel SJ, Whigham A, Hakim A, Pettigrew RI, Oshinski JN. Three-dimensional, time-resolved motion of the coronary arteries. J Cardiovasc Magn Reson. 2004. 6:663–673.5. Wang Y, Watts R, Mitchell I, Nguyen TD, Bezanson JW, Bergman GW, et al. Coronary MR angiography: selection of acquisition window of minimal cardiac motion with electrocardiography-triggered navigator cardiac motion prescanning--initial results. Radiology. 2001. 218:580–585.6. Hofman MB, Wickline SA, Lorenz CH. Quantification of inplane motion of the coronary arteries during the cardiac cycle: implications for acquisition window duration for MR flow quantification. J Magn Reson Imaging. 1998. 8:568–576.7. Wang Y, Vidan E, Bergman GW. Cardiac motion of coronary arteries: variability in the rest period and implications for coronary MR angiography. Radiology. 1999. 213:751–758.8. Finn JP, Nael K, Deshpande V, Ratib O, Laub G. Cardiac MR imaging: state of the technology. Radiology. 2006. 241:338–354.9. Deshpande VS, Shea SM, Laub G, Simonetti OP, Finn JP, Li D. 3D magnetization-prepared true-FISP: a new technique for imaging coronary arteries. Magn Reson Med. 2001. 46:494–502.10. Giorgi B, Dymarkowski S, Maes F, Kouwenhoven M, Bogaert J. Improved visualization of coronary arteries using a new three-dimensional submillimeter MR coronary angiography sequence with balanced gradients. AJR Am J Roentgenol. 2002. 179:901–910.11. Spuentrup E, Buecker A, Stuber M, Botnar R, Nguyen TH, Börnert P, et al. Navigator-gated coronary magnetic resonance angiography using steady-state-free-precession: comparison to standard T2-prepared gradient-echo and spiral imaging. Invest Radiol. 2003. 38:263–268.12. Gerber BL, Coche E, Pasquet A, Ketelslegers E, Vancraeynest D, Grandin C, et al. Coronary artery stenosis: direct comparison of four-section multi-detector row CT and 3D navigator MR imaging for detection--initial results. Radiology. 2005. 234:98–108.13. Sakuma H, Ichikawa Y, Suzawa N, Hirano T, Makino K, Koyama N, et al. Assessment of coronary arteries with total study time of less than 30 minutes by using whole-heart coronary MR angiography. Radiology. 2005. 237:316–321.14. Nehrke K, Börnert P, Mazurkewitz P, Winkelmann R, Grasslin I. Free-breathing whole-heart coronary MR angiography on a clinical scanner in four minutes. J Magn Reson Imaging. 2006. 23:752–756.15. Stehning C, Börnert P, Nehrke K, Eggers H, Stuber M. Free-breathing whole-heart coronary MRA with 3D radial SSFP and self-navigated image reconstruction. Magn Reson Med. 2005. 54:476–480.16. Tang L, Merkle N, Schär M, Korosoglou G, Solaiyappan M, Hombach V, et al. Volume-targeted and whole-heart coronary magnetic resonance angiography using an intravascular contrast agent. J Magn Reson Imaging. 2009. 30:1191–1196.17. Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, et al. ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J Am Coll Cardiol. 1999. 33:1756–1824.18. Stuber M, Botnar RM, Fischer SE, Lamerichs R, Smink J, Harvey P, et al. Preliminary report on in vivo coronary MRA at 3 Tesla in humans. Magn Reson Med. 2002. 48:425–429.19. Zagrosek A, Noeske R, Abdel-Aty H, Friedrich MG, Dietz R, Schulz-Menger J. MR coronary angiography using 3D-SSFP with and without contrast application. J Cardiovasc Magn Reson. 2005. 7:809–814.20. Niendorf T, Hardy CJ, Giaquinto RO, Gross P, Cline HE, Zhu Y, et al. Toward single breath-hold whole-heart coverage coronary MRA using highly accelerated parallel imaging with a 32-channel MR system. Magn Reson Med. 2006. 56:167–176.21. Ohnesorge B, Flohr T, Becker C, Kopp AF, Schoepf UJ, Baum U, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology. 2000. 217:564–571.22. Weissler AM, Harris WS, Schoenfeld CD. Systolic time intervals in heart failure in man. Circulation. 1968. 37:149–159.23. Gharib AM, Herzka DA, Ustun AO, Desai MY, Locklin J, Pettigrew RI, et al. Coronary MR angiography at 3T during diastole and systole. J Magn Reson Imaging. 2007. 26:921–926.24. Plein S, Jones TR, Ridgway JP, Sivananthan MU. Three-dimensional coronary MR angiography performed with subject-specific cardiac acquisition windows and motion-adapted respiratory gating. AJR Am J Roentgenol. 2003. 180:505–512.25. Iozzelli A, D'Orta G, Aliprandi A, Secchi F, Di Leo G, Sardanelli F. The value of true-FISP sequence added to conventional gadolinium-enhanced MRA of abdominal aorta and its major branches. Eur J Radiol. 2009. 72:489–493.26. Pereles FS, McCarthy RM, Baskaran V, Carr JC, Kapoor V, Krupinski EA, et al. Thoracic aortic dissection and aneurysm: evaluation with nonenhanced true FISP MR angiography in less than 4 minutes. Radiology. 2002. 223:270–274.27. Krishnam MS, Tomasian A, Malik S, Desphande V, Laub G, Ruehm SG. Image quality and diagnostic accuracy of unenhanced SSFP MR angiography compared with conventional contrast-enhanced MR angiography for the assessment of thoracic aortic diseases. Eur Radiol. 2010. 20:1311–1320.28. Bi X, Li D. Coronary arteries at 3.0 T: Contrast-enhanced magnetization-prepared three-dimensional breathhold MR angiography. J Magn Reson Imaging. 2005. 21:133–113.29. Bi X, Carr JC, Li D. Whole-heart coronary magnetic resonance angiography at 3 Tesla in 5 minutes with slow infusion of Gd-BOPTA, a high-relaxivity clinical contrast agent. Magn Reson Med. 2007. 58:1–7.30. Sommer T, Hackenbroch M, Hofer U, Schmiedel A, Willinek WA, Flacke S, et al. Coronary MR angiography at 3.0 T versus that at 1.5 T: initial results in patients suspected of having coronary artery disease. Radiology. 2005. 234:718–725.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breath-Hold MR Imaging of Focal Hepatic Lesions: Clinical Usefulness of Breath-Hold TSE T2WI Combined by FastLow-Angle Shot (FLASH) MR Imaging
- Comparison of Gadolinium Polylysine and Gadopentetate in Contrast Enhanced MR Imaging of IVlyocardial Ischemia-Reperfusion in Cats
- Detection of Acute Intraventricular Hemorrhage: Comparison of FLAIR MR Imaging with Unenhanced CT
- Hepatic Enhancement on Gd-BOPTA-enhanced MR Imaging: Comparison between Cirrhotic and Normal Livers
- Contrast-enhanced Magnetic Resonance Imaging of Brain Metastases at 7.0T versus 1.5T: A Preliminary Result
