Fibrovascularization of Intraorbital Hydroxyapatite-Coated Alumina Sphere in Rabbits
- Affiliations
-
- 1Dr. Chung's Eye Clinic, Taegu, Korea. eye-chung@hanmail.net
- 2Department of Ophthalmology, College of Medicine, Seoul National University, Seoul, Korea.
- 3Department of Ophthalmology, College of Medicine, Yeungnam University, Taegu, Korea.
- KMID: 1099079
- DOI: http://doi.org/10.3341/kjo.2005.19.1.9
Abstract
- We investigated the fibrovascular ingrowth and fibrovascular tissue maturation of hydroxyapatite-coated, porous alumina sphere (Alumina sphere) in comparison with the hydroxyapatite sphere (HAp sphere) in rabbits. Alumina spheres and HAp spheres were implanted in the left orbits of 42 New Zealand white rabbits after enucleation. Fibrovascular ingrowth and maturation were graded from 1 to 5 at postoperative 1, 2, 3, 4, 8, 12 and 24 weeks. We defined 4 phases: postoperative 1-2 weeks as phase I, 3-4 weeks as phase II, 8-12 weeks as phase III, and 24 weeks as phase IV. The grade was analyzed at each phases. There was no significant difference in fibrovascular ingrowth and maturation between the two groups at all 4 phases, except phase II at which the Alumina sphere showed significantly lower maturation grade (p< 0.05). We concluded that the Alumina sphere is an ideal orbital implant material and an ideal substitute for the HAp sphere in clinical practice.
Keyword
MeSH Terms
Figure
-
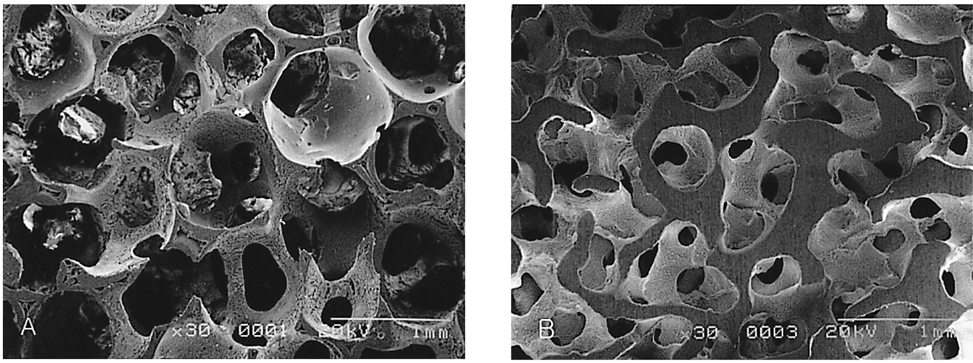
Fig. 1 Scanning electron micrograph of hydroxyapatite-coated alumina sphere and hydroxyapatite sphere. (A) Hydroxyapatite-coated alumina sphere shows porosity of 90% and pore size of 500-600 µm. (B) Hydroxyapatite sphere shows porosity of 60-70% and pore size of 300-500 µm.
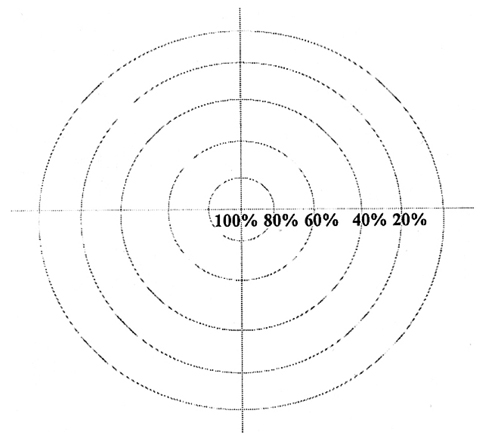
Fig. 2 Schematic diagram for grading of fibrovascular ingrowth.
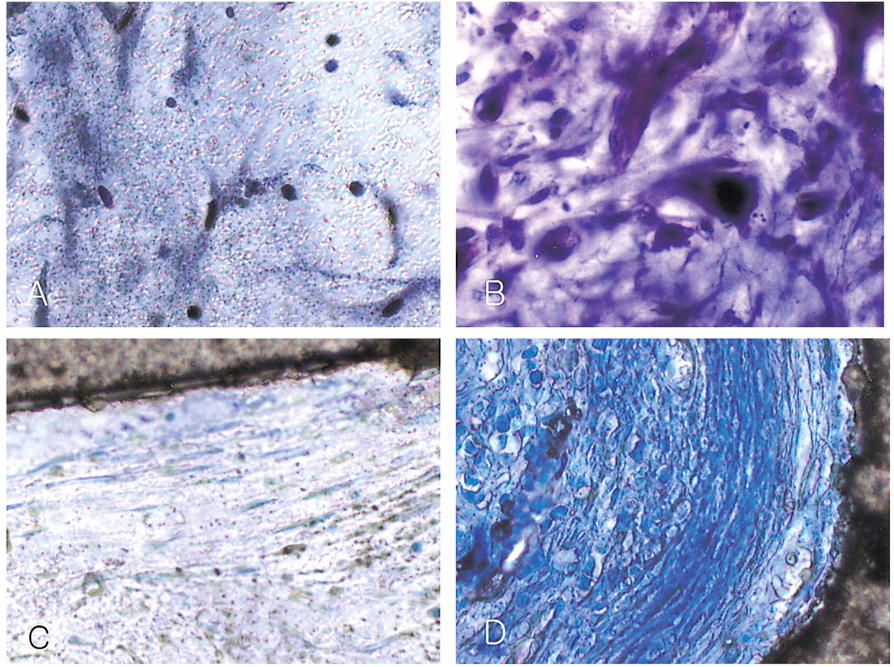
Fig. 3 Fibrovascular maturation grades of the hydroxyapatite-coated alumina sphere. (A) Maturation grade 1 shows edematous young granulation tissue and little fibroblast proliferation (Toluidine blue stain, ×200). (B) Maturation grade 2 shows moderate fibroblast proliferation and decreased edema. (Toluidine blue stain, ×400). (C) Maturation grade 3 shows early stage of collagen fiber lay-down. (Toluidine blue stain, ×200). (D) The granulation tissue is composed of collagen fibers in almost all areas in grade 5. (Toluidine blue stain, ×200).
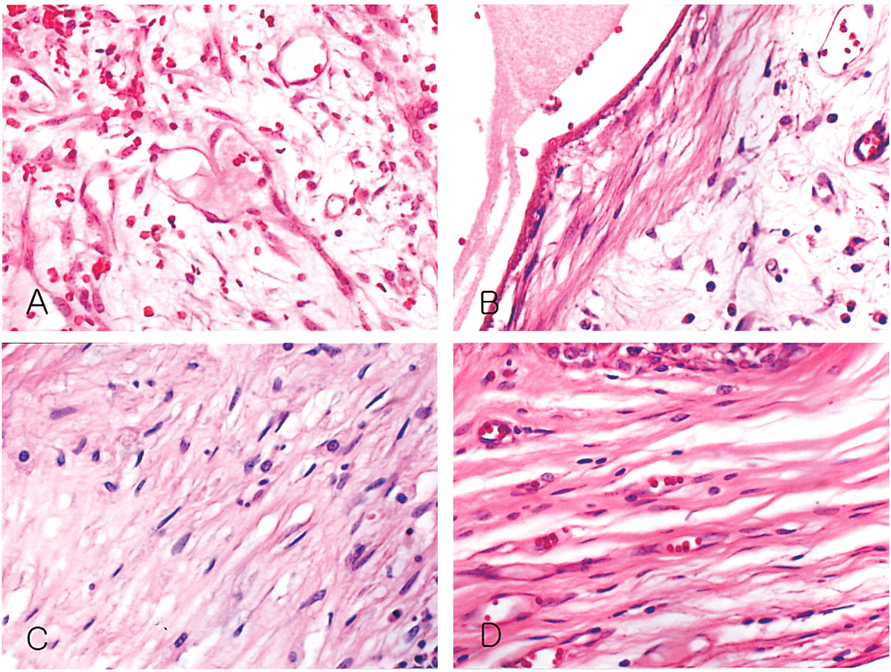
Fig. 4 Fibrovascular maturation grades of the hydroxyapatite sphere (hematoxylin-eosin stain, ×200). (A) Maturation grade 2 shows fibroblast proliferation and capillary development in the edematous stroma. A few neutrophils are present. (B) Collagen fiber lay-down is initiated in grade 3. (C) Marked increase of collagen is noted in grade 4. (D) In grade 5, there is compact growth of collagen fibers.
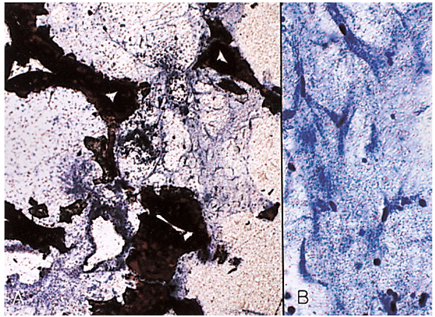
Fig. 5 Hydroxyapatite-coated alumina sphere at postoperative 1 week. (A) Fibrovascular ingrowth accounts for about 20% of the radius of implant in grade 1 (periphery of the implant, Toluidine blue stain, ×40). (B) Fibroblasts begin to proliferate in grade 1 (Toluidine blue stain, ×200).
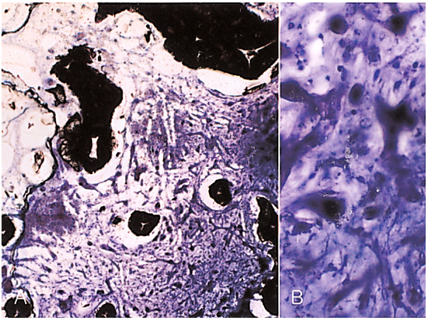
Fig. 6 Hydroxyapatite-coated alumina sphere at postoperative 2 weeks. (A) Fibrovascular ingrowth accounts for about 40% of the radius of implant in grade 2 (periphery of the implant, Toluidine blue stain, ×40). (B) Fibroblast proliferation is considered as grade 2 (Toluidine blue stain, ×200).
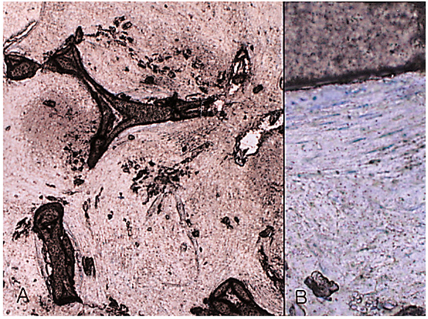
Fig. 7 Hydroxyapatite-coated alumina sphere at postoperative 3 weeks. (A) Fibrovascular proliferation reaches the central portion of the implant (center of the implant, Toluidine blue stain, ×40). (B) The implant shows initial stage of collagen lay-down, representing maturation grade 3 (Toluidine blue stain, ×200).
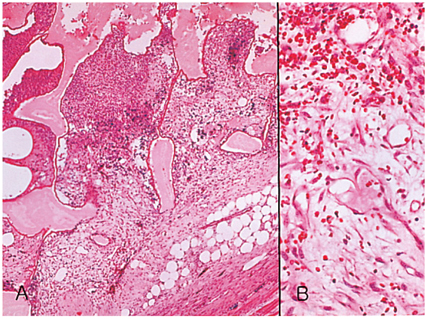
Fig. 8 Hydroxyapatite sphere at postoperative 1 week. (A) Fibrovascular ingrowth accounts for about 20% of the radius of implant in grade 1 (periphery of the implant, Hematoxylin-eosin stain, ×40). (B) Moderate fibroblast proliferation and considerable capillary proliferation indicates grade 2 (Hematoxylin-eosin stain, ×200).
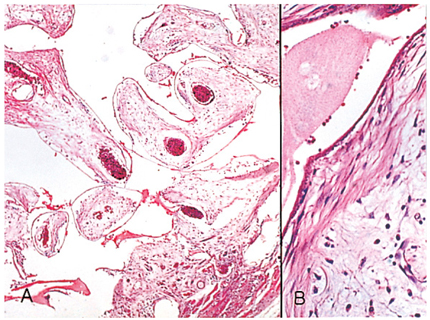
Fig. 9 Hydroxyapatite sphere at postoperative 2 weeks. (A) Fibrovascular ingrowth accounts for about 60% of the radius of implant in grade 3 (periphery of the implant, Hematoxylin-eosin stain, ×40). (B) The implant shows the initial stage of collagen fiber lay-down, representing grade 3 maturation (Hematoxylin-eosin stain, ×200).
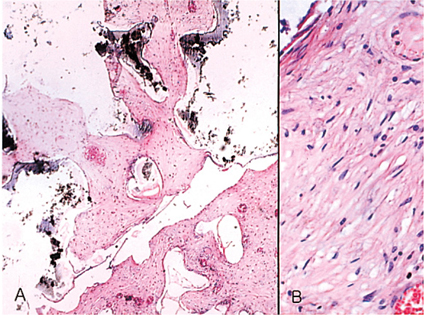
Fig. 10 Hydroxyapatite sphere at postoperative 3 weeks. (A) The central portion of the implant is filled with fibrovascular proliferation, representing grade 5 (center of the implant, Hematoxylin-eosin stain, ×40). (B) The granulation tissue is composed of collagen fibers in almost all areas in grade 5 (Hematoxylin-eosin stain, ×200).
Reference
-
1. Durham DG. The new ocular implants. Am J Ophthalmol. 1949. 32:79–89.2. Shields CL, Shields JA, De Potter P. Hydroxyapatite orbital implant after enucleation: experience with initial 100 consecutive cases. Arch Ophthalmol. 1992. 110:333–338.3. Rubin PA, Nicaeus TE, Warner MA, Remulla HO. Effect of sucralfate and basic fibroblast growth factor on fibrovascular ingrowth into hydroxyapatite and porous polyethylene alloplastic implants using novel rabbit model. Ophthal Plast Reconstr Surg. 1997. 13:8–17.4. Byrd WA. Coraline hydroxyapatite orbital implant. Ophthal Practice. 1991. 9:262–266.5. Cutton JJ. Coraline hydroxyapatite as an ocular implant. Ophthalmology. 1991. 98:370–377.6. Perry AR. Advances in enucleation. Ophthal Plast Reconstr Surg. 1991. 4:173–182.7. Roy DM, Linnehan SK. Hydroxyapatite formed from coral skeletal carbonate by hydrothermal exchange. Nature. 1974. 247:220–222.8. You CK, Oh SH, Kim SY. Hydroxyapatite coated porous alumina as a new orbital implant. Key Engineering Materials. 2003. 240–242. 563–566.9. Hornblass A, Biesman B, Eviatar J. Current techniques of enucleation: a summary of 5439 intraorbital implants and a review of the literature. Ophthal Plast Reconstr Surg. 1995. 11:77–88.10. Fricain J, Baquei C, Dupuy B. Resorption of corals implanted in diffusion chambers. J Mater Sci Mater Med. 1995. 6:680–684.11. Mawn LA, Jordan DR, Gilberg S. Scanning electron microscopic examination of porous orbital implants. Can J Ophthalmol. 1998. 33:203–209.12. Jordan DR, Mawn LA, Brownstein S, et al. The bioceramic orbital implant: a new generation of porous implants. Ophthal Plast Reconstr Surg. 2000. 16:347–355.13. Jordan DR, Gilberg S, Mawn LA. The bioceramic orbital implant. Experience with 107 implants. Ophthal Plast Reconstr Surg. 2003. 19:128–135.14. Bose MO, Avers RJ, Rieger MR, Duckworth JE. Submerged alumina dental root implants in humans: five-year evaluation. J Prosthet Dent. 1989. 61:594–601.15. Sclatter C. Biomedical aspects of aluminum. Med Lav. 1992. 83:470–474.16. Heimke G, Griss P, Jentschura G, Werner E. Bioinert and bioactive ceramics in orthopaedic surgery. Mechanical properties of biomaterials. 1980. Toronto: John Willey & Sons;207–215.17. Labat B, Chamson A, Frey J. Effects of γ-alumina and hydroxyapatite coatings on the growth and metabolism of human osteoblasts. J Biomed Mater Res. 1995. 29:1397–1401.18. Rubin PA, Popham JK, Bilyk JR, Shore JW. Comparison of fibrovascular ingrowth into hydroxyapatite and porous polyethylene orbital implants. Ophthal Plast Reconstr Surg. 1994. 10:96–103.19. Rubin PA, Bilyk JR, Shore JW. Orbital reconstruction using porous polyethylene sheets. Ophthalmology. 1994. 101:1697–1708.20. Seong YS, Lee SY, Kim SJ. Morphological study of a new orbital implant: hydroxyapatite-coated porous alumina in rabbit. J Korean Ophthalmol Soc. 2001. 42:1354–1361.21. Jordan DR, Brownstein S, Gilberg S, et al. Hydroxyapatite and calcium phosphate coatings on aluminium oxide orbital implants. Can J Ophthalmol. 2001. 37:7–13.22. Mawn LA, Jordan DR, Gilberg S. Scanning electron microscopic examination of porous orbital implants. Can J Ophthalmol. 1998. 33:203–209.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Morphological Study of a New Orbital Implant: Hydroxyapatite-Coated Porous Alumina in Rabbit
- Fibrovascular Ingrowth of the Orbital Hydroxyapatite Implant evaluated by Magnetic Resonance Imaging
- MRI Findings of Orbital Hydroxyapatite Implants in Postoperative 5 months
- Effect of Collagen Gel with Growth Factor and Wrapping Materials on Fibrovascularization of Porous Orbital Implant
- Histopathologic Comparison of Vascularization between Dacron and Donor Sclera as Wrapping Material in Hydroxyapatite Implantation
