Hydatid Disease Involving Some Rare Locations in the Body: a Pictorial Essay
- Affiliations
-
- 1KSU Medical School Department of Radiology 46050 Kahramanmaras-Turkey. myuksel@ksu.edu.tr
- 2Ege University Medical School Department of Radiology 35100 Izmir-Turkey.
- 3KSU Medical School Department of Pathology 46050 Kahramanmaras-Turkey.
- 4KSU Medical School Department of General Surgery 46050 Kahramanmaras-Turkey.
- KMID: 1089441
- DOI: http://doi.org/10.3348/kjr.2007.8.6.531
Abstract
- Hydatid disease (HD) is an endemic illness in many countries, and it poses an important public health problem that's influenced by peoples' socioeconomic status and migration that spreads this disease. Although rare, it may occur in any organ or tissue. The most common site is the liver (59-75%), followed in frequency by lung (27%), kidney (3%), bone (1-4%) and brain (1-2%). Other sites such as the heart, spleen, pancreas and muscles are very rarely affected. Unusual sites for this disease can cause diagnostic problems. This pictorial essay illustrates various radiological findings of HD in the liver, spleen, kidney, pancreas, peritoneal cavity, omentum, adrenal, ovary, lung, mediastinum and retroperitoneum. Familiarity with the imaging findings of HD may be helpful in making an accurate diagnosis and preventing potential complications.
MeSH Terms
-
Abdominal Cavity/parasitology/radiography
Adolescent
Adult
Child
Child, Preschool
Contrast Media/administration & dosage
Digestive System/pathology/radiography/ultrasonography
Digestive System Diseases/diagnosis/parasitology
Echinococcosis/*diagnosis/parasitology/*radiography
Endocrine Glands/parasitology/radiography
Female
Humans
Kidney/parasitology/pathology
Liver/parasitology/radiography
Lung/parasitology/radiography
Magnetic Resonance Imaging/methods
Male
Mediastinum/parasitology/radiography
Middle Aged
Pancreas/parasitology/radiography
Radiographic Image Enhancement/methods
Spleen/parasitology/radiography
Tomography, X-Ray Computed/methods
Figure
-
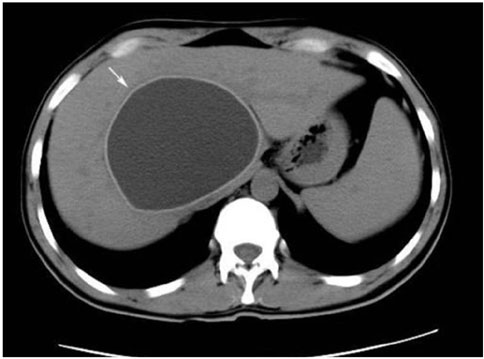
Fig. 1 Type I hydatid cyst of the liver in an 11-year-old girl. Unenhanced CT scan of the upper abdomen shows a large unilocular hydatid cyst (18 HU) with a high-attenuation wall in the subdiaphragmatic portion of the liver (arrow).

Fig. 2 Type II hydatid cyst in a 36-year-old man. Contrast-enhanced axial CT scan of the upper abdomen demonstrates cystic lesion with peripheral daughter cysts and wall calcification in the left lobe of the liver. Note the daughter cysts have a lower attenuation value than the mother cyst (arrows).

Fig. 3 Type III hydatid cyst in a 28-year-old man. Densely calcified lesion is seen on the right upper quadrant of the abdomen on barium radiography of the stomach.
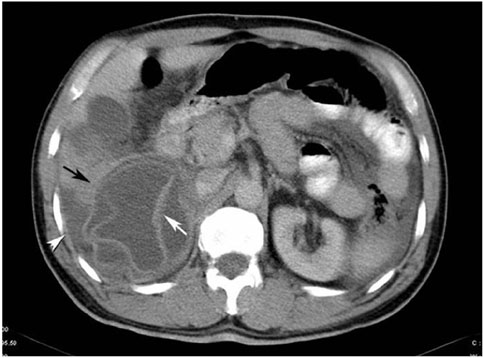
Fig. 4 Direct rupture of hydatid cyst into the peritoneal cavity in a 50-year-old man. Contrast-enhanced axial CT scan of the upper abdomen demonstrates a partially collapsed cystic lesion (black arrow) with an irregular contour growing exophytically from the liver. It has lost its normal spherical shape. Isoattenuating detached membranes (white arrow) appear as serpentine structures within the lesion. A small amount of ascites (white arrowhead) is present.
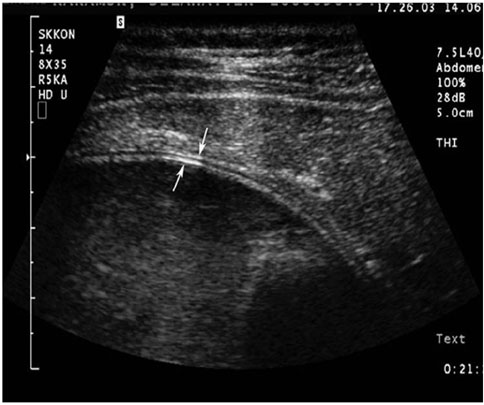
Fig. 5 Type I hydatid cyst of the liver in a 42-year-old woman. At US examination of liver, the cyst wall is seen as double echogenic lines separated by a hypoechoic layer (the double-line sign) (small white arrows). This finding helps to differentiate hydatid cysts from simple cysts, cystic tumors, pseudocysts or metastases.

Fig. 6 Type II hydatid cyst is seen on US examination of the liver in a 37-year-old man. Multiple echogenic sand (small white arrows), which is composed of brood capsules and scolices, falls to the dependent portion of the cyst by repositioning the patient. This finding is referred to as the snowstorm sign. Note the early separation of the laminated membrane from the germinal membrane (large white arrow).
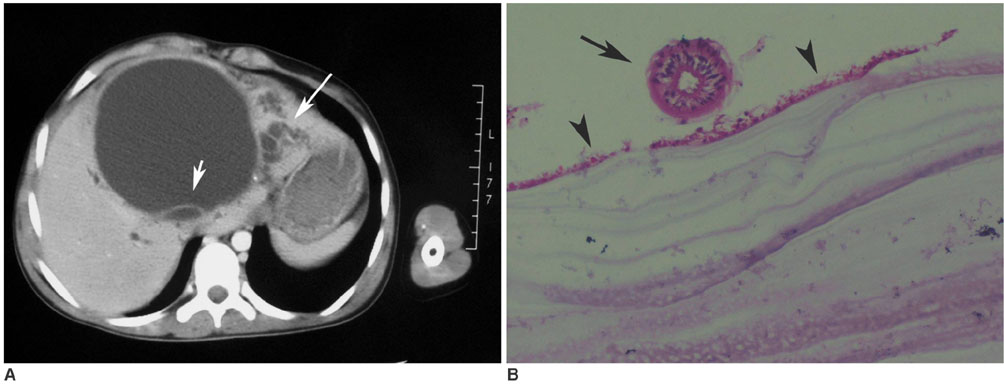
Fig. 7 A. Large type II hydatid cyst of the liver in a 12-year-old girl. Contrast-enhanced transverse CT scan of the upper abdomen demonstrates cystic lesion with a peripheral daughter cyst (short arrow). There is also evidence of pericystic biliary ducts dilatation secondary to the mass effect by a large echinococcal cyst (long arrow). B. Microscopic section of hydatid cyst in the same patient shows a laminated membrane that is lined inside by the germinal layer (arrowheads). There is also a scolex (arrow) close to the germinal layer. (Hematoxylin & Eosin staining; original magnification × 10)
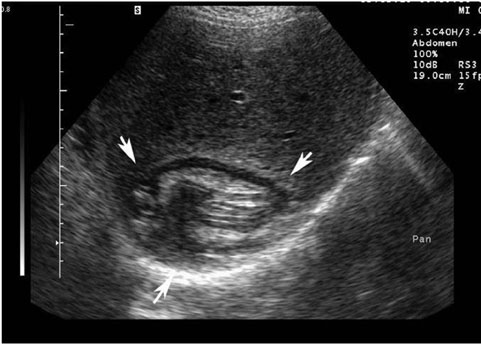
Fig. 8 Type II hydatid cyst mimicking a solid mass in a 25-year-old man. US image demonstrates a mixed echogenic lesion (arrows) of the liver. Note the serpentine structures within the matrix, which represents the collapsed membranes.
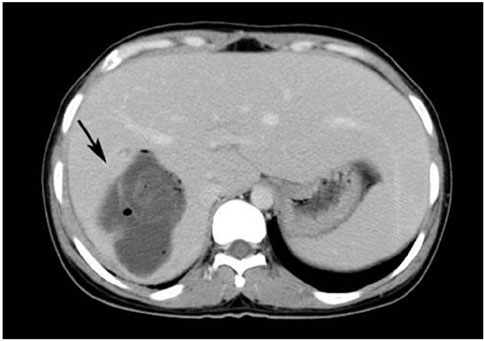
Fig. 9 Infected hydatid cyst of the liver in a 25-year-old woman. Contrast-enhanced CT scan shows a cystic lesion, including air bubbles and collapsed membranes, in the right lobe of the liver (black arrow).
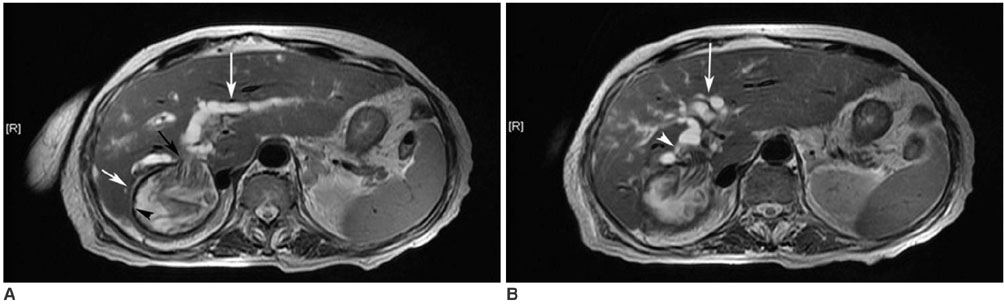
Fig. 10 Rupture of hydatid cyst into the biliary tree in a 54-year-old woman. A, B. The axial MR image of the upper abdomen using a fast spin-echo T2-weighted sequence shows a hyperintense cystic lesion (short white arrow), including hypointense linear structures representing detached membranes, in the right lobe of liver. There is the hypointense rim (black arrowhead) at the periphery of the lesion. MRI reveals cyst wall defect (black arrow) and the passage of detached membranes through a defect into the extrahepatic bile duct (white arrowhead). Note the biliary dilatation (long white arrows) due to obstruction of the extrahepatic bile duct by hydatid membranes.

Fig. 11 Portal vein involvement of hydatid disease in a 20-year-old woman. The axial (A) contrast enhanced spin-echo T1-weighted sequence (fat-suppression technique) shows a low-signal-intensity lesion in the subdiaphragmatic portion of the right hepatic lobe (white arrow). Thrombosis is identified within the branches of the portal vein (small black arrows). On MR angiography (B), portosystemic venous collaterals (white arrowhead) are seen and the portal vein is not visualized.

Fig. 12 Multiple lung hydatid cysts in a 30-year-old woman. Axial contrast-enhanced CT of the thorax shows multiple type I hydatid cysts in the lung. There are also ruptured hydatid cysts in the lower lobe of the right lung with the inverse crescent sign (arrow) due to air between the endocyst and pericyst.
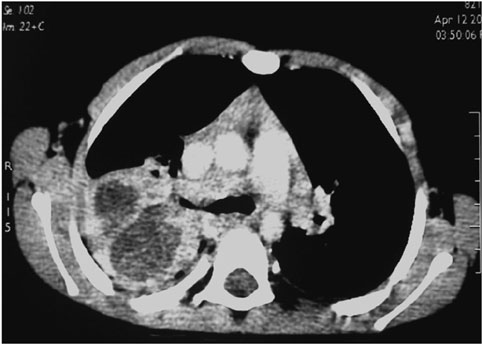
Fig. 13 Infected pulmonary hydatid cyst in a 5-year-old boy. Axial contrast-enhanced CT scan with a mediastinal window setting shows multiloculated low-attenuation lesion with a thick wall in the right lung.
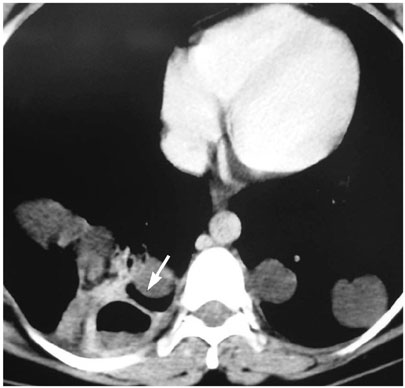
Fig. 14 A 44-year-old-man with type II hydatid cyst of the left kidney. After albendazole therapy, detached germinal membranes are seen within the cyst as low signal intensity linear structures on coronal T2-weighted spin-echo MRI (white arrow).

Fig. 15 Intraperitoneal hydatid cyst in a 40-year-old woman with a history of liver involvement and previous surgery. The contrast-enhanced axial CT scan revealed multiple cystic lesions (arrows) and ascites (asterisk) in the pelvis.
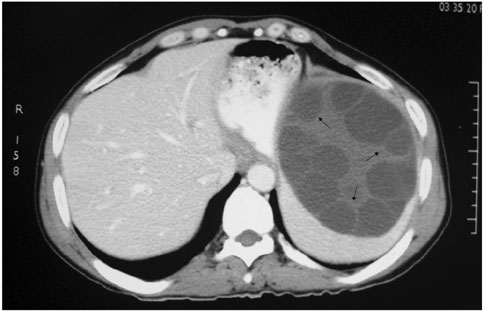
Fig. 16 Large type II hydatid cyst with primary splenic involvement in a 50-year-old woman. Contrast-enhanced axial CT scan of the abdomen demonstrates unenhanced, well-defined hypodense lesion with a hydatid matrix and peripheral daughter cysts (arrows) in the upper part of the spleen.
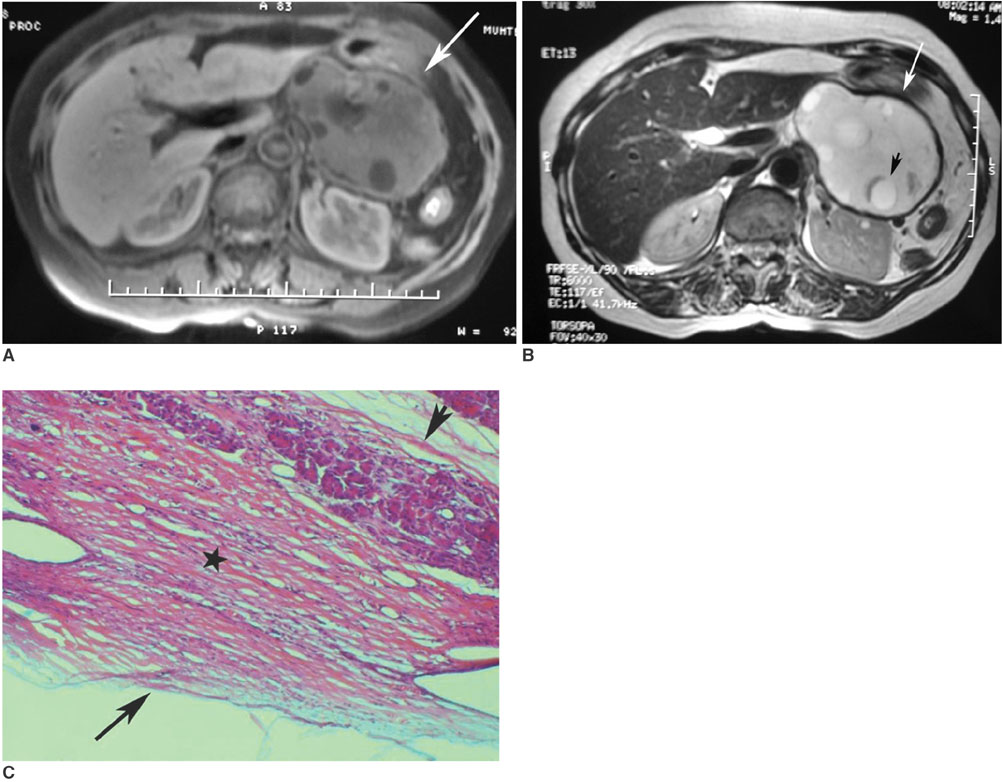
Fig. 17 Type II hydatid cyst with primary pancreas involvement in a 57-year-old woman. A. Axial MR image of the upper abdomen shows low-signal-intensity lesion with peripheral daughter cysts on the T1-weighted sequence (fat-suppression technique) (arrow). Daughter cysts are seen as lower-signal-intensity lesions compared to the mother cyst. B. On axial MR image of the upper abdomen, daughter cysts are seen within the mother cyst (short black arrow). The mother cyst and daughter cysts are seen as hyperintense lesions on the fast spin-echo T2-weighted sequence. Also note the hypointense rim at the periphery of the lesion (long white arrow). C. Microscopic section of hydatid cyst following distal pancreatectomy demonstrates a thick laminated membrane (star) with a thin germinal layer (long arrow). Short arrow shows the pancreas parenchyma.
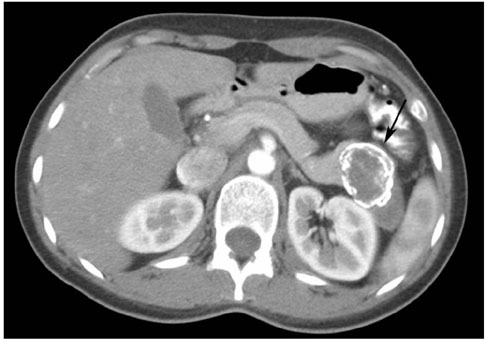
Fig. 18 Partially calcified hydatid cyst of the pancreas in a 27-year-old woman. Contrast material-enhanced CT scan shows a hypodense lesion with dense peripheral calcification (arrow) in the tail of the pancreas.

Fig. 19 Type II hydatid cyst of the right adrenal gland in a 47-year-old woman. The axial (A) spin echo T1-weighted MR image demonstrates low-signal-intensity hydatid cyst with peripheral daughter cysts (arrows) in the right adrenal gland. Note that the daughter cysts have lower signal intensity compared to the mother cyst. The sagittal (B) plane spin echo T2-weighted MR image shows linear structures within the mother cyst, which represent detached membranes (long black arrow), and round, nodular lesions within the mother cyst, which represent daughter cysts (short black arrows).
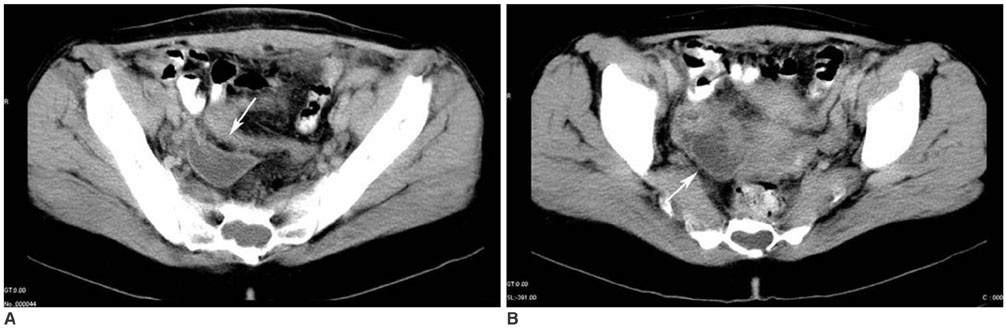
Fig. 20 Incidentally found type I hydatid cyst of the ovary in a 39-year-old woman. The axial (A, B) contrast-enhanced CT scan shows a unilocular low-attenuation lesion (arrows) in the right ovary.

Fig. 21 Type II retroperitoneal hydatid cyst in a 25-year-old woman. The axial contrast-enhanced CT scan through the pelvis demonstrates a hydatid cyst with daughter cysts (arrow) adjacent to the right psoas muscle.
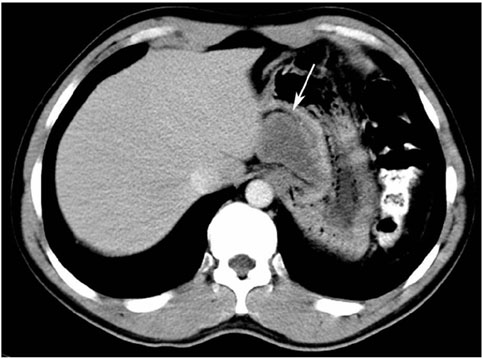
Fig. 22 An omental hydatid disease in a 36-year-old man. The axial contrast-enhanced CT scan obtained through the stomach shows unilocular low-attenuation lesion (arrow) in the lesser omentum, which represents type I hydatid cyst.
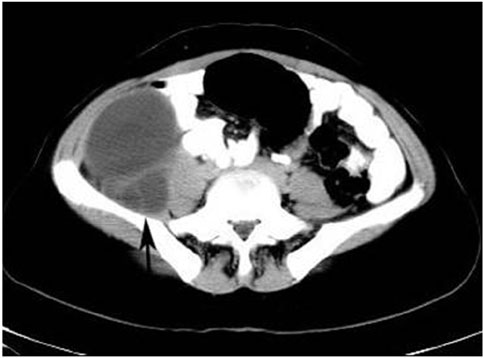
Fig. 23 A mediastinal hydatid disease in a 20-year-old man. The axial contrast-enhanced CT scan shows a well-defined, low-attenuation lesion (arrow) that is consistent with type I unilocular hydatid cyst. Compression of the superior vena cava by the hydatid cyst is also seen.
Reference
-
1. Lewall DB. Hydatid disease: biology, pathology, imaging and classification. Clin Radiol. 1998. 53:863–874.2. Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003. 23:475–494.3. Pedrosa I, Saiz A, Arrazola J, Ferreiros J, Pedrosa CS. Hydatid disease: radiologic and pathologic features and complications. Radiographics. 2000. 20:795–817.4. Czermak BV, Unsinn KM, Gotwald T, Niehoff AA, Freund MC, Waldenberger P, et al. Echinococcus granulosus revisited: radiologic patterns seen in pediatric and adult patients. AJR Am J Roentgenol. 2001. 177:1051–1056.5. Beggs I. The radiology of hydatid disease. AJR Am J Roentgenol. 1985. 145:639–648.6. Erdem LO, Erdem CZ, Karlioguz K, Uner C. Radiologic aspects of abdominal hydatidosis in children: a study of 31 cases in Turkey. Clin Imaging. 2004. 28:196–200.7. Papageorgiou KI, Kaniorou-Larai M, Mathew RG. An unusual presentation of hydatid cyst within the soft tissues of the back: re-investigation of the undiagnosed lung opacity. Respir Med. 2005. 99:1191–1194.8. Von Sinner W, te Strake L, Clark D, Sharif H. MR imaging in hydatid disease. AJR Am J Roentgenol. 1991. 157:741–745.9. Haddad MC, Birjawi GA, Khouzami RA, Khoury NJ, El-Zein YR, Al-Kutoubi AO. Unilocular hepatic echinococcal cysts: sonography and computed tomography findings. Clin Radiol. 2001. 56:746–750.10. Kiresi DA, Karabacakoglu A, Odev K, Karakose S. Uncommon locations of hydatid cysts. Acta Radiol. 2003. 44:622–636.11. Koul PA, Koul AN, Wahid A, Mir FA. CT in pulmonary hydatid disease: unusual appearances. Chest. 2000. 118:1645–1647.12. Escudero MD, Sabater L, Calvete J, Camps B, Labios M, Lledo S. Arterial hypertension due to primary adrenal hydatid cyst. Surgery. 2002. 132:894–895.13. Dahniya MH, Hanna RM, Ashebu S, Muhtaseb SA, el-Beltagi A, Badr S, et al. The imaging appearances of hydatid disease at some unusual sites. Br J Radiol. 2001. 74:283–289.14. Canda MS, Guray M, Canda T, Astarcioglu H. The pathology of echinococcosis and the current echinococcosis problem in western turkey (a report of pathologic features in 80 cases). Turk J Med Sci. 2003. 33:369–374.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hepatic Hydatid Disease Causing Gastric Ulcer as a Rare Complication
- Double Retroperitoneal Hydatid Localization: A Case Report
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Systemic Manifestations of Immunoglobulin G4-Related Disease: A Pictorial Essay
- Multi-Detector CT Findings of Typical and Atypical Appendicitis: A Pictorial Essay
