The Short-Term Effects of Balloon-Occluded Retrograde Transvenous Obliteration, for Treating Gastric Variceal Bleeding, on Portal Hypertensive Changes: a CT Evaluation
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. swshin@smc.samsung.co.kr
- 2Department of Radiology, Kangwon National University College of Medicine, Kangwon-do, Korea.
- KMID: 1089440
- DOI: http://doi.org/10.3348/kjr.2007.8.6.520
Abstract
- OBJECTIVE: We wanted to evaluate the short-term effects of balloon-occluded retrograde transvenous obliteration (BRTO) for treating gastric variceal bleeding, in terms of the portal hypertensive changes, by comparing CT scans. MATERIALS AND METHODS: We enrolled 27 patients who underwent BRTO for gastric variceal bleeding and they had CT scans performed just before and after BRTO. The pre- and post-procedural CT scans were retrospectively compared by two radiologists working in consensus to evaluate the short-term effects of BRTO on the subsequent portal hypertensive changes, including ascites, splenomegaly, portosystemic collaterals (other than gastrorenal shunt), the gall bladder (GB) edema and the intestinal wall edema. Statistical differences were analyzed using the Wilcoxon signed rank test and the paired t-test. RESULTS: Following BRTO, ascites developed or was aggravated in 22 (82%) of 27 patients and it was improved in two patients; the median spleen volumes increased from 438.2 cm3 to 580.8 cm3, and based on a 15% volume change cut-off value, splenic enlargement occurred in 15 (56%) of the 27 patients. The development of new collaterals or worsening of existing collaterals was not observed in any patient. GB wall edema developed or was aggravated in four of 23 patients and this disappeared or improved in five; intestinal wall edema developed or was aggravated in nine of 27 patients, and this disappeared or improved in five. Statistically, we found significant differences for ascites and the splenic volumes before and after BRTO (p = 0.001 and p < 0.001, respectively) CONCLUSION: Some portal hypertensive changes, including ascites and splenomegaly, can be aggravated shortly after BRTO.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Ascites/diagnosis/etiology
Balloon Occlusion/adverse effects/*methods
Cholecystography
Contrast Media/administration & dosage
Edema/diagnosis/etiology
Esophageal and Gastric Varices/complications/*therapy
Female
Follow-Up Studies
Gastrointestinal Hemorrhage/etiology/*therapy
Humans
Hypertension, Portal/*diagnosis/etiology
Intestines/radiography
Iohexol/analogs & derivatives/diagnostic use
Liver Cirrhosis/complications
Male
Middle Aged
Observer Variation
Organ Size
Retrospective Studies
Spleen/radiography
Splenomegaly/diagnosis/etiology
Time Factors
Tomography, X-Ray Computed/*methods
Treatment Outcome
Figure
-
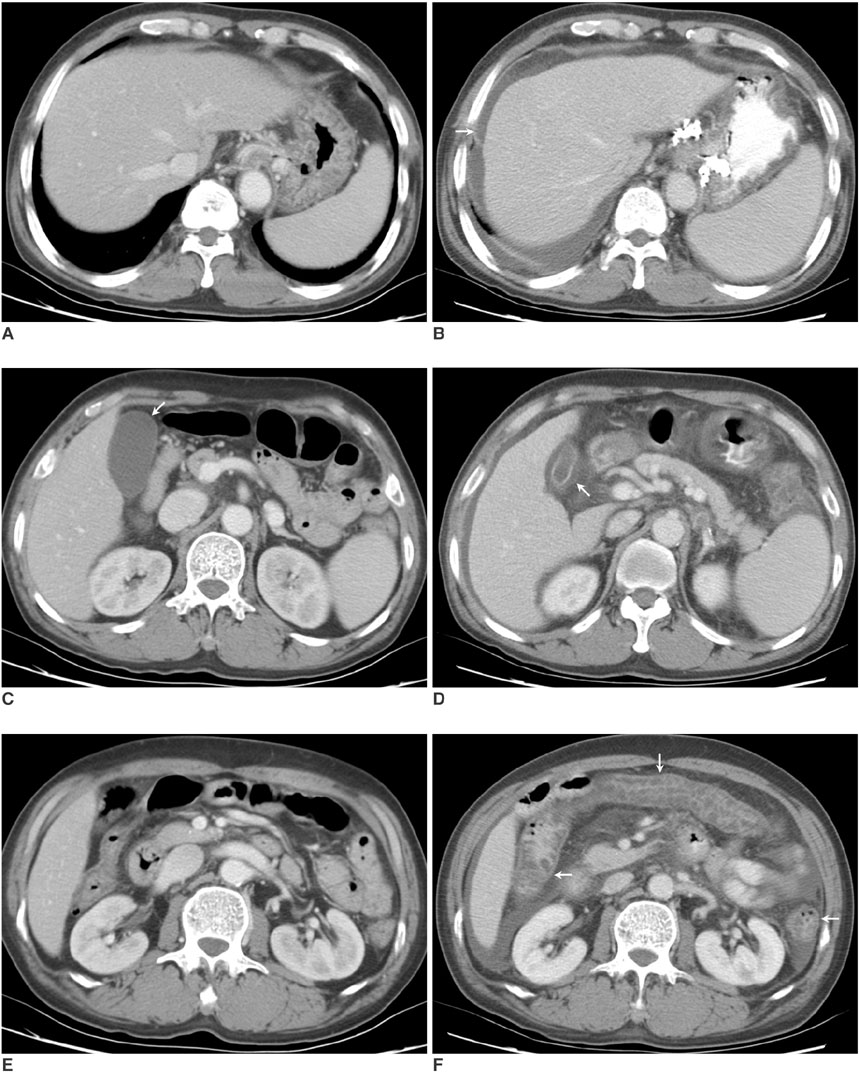
Fig. 1 Patient 13. A 63-year-old man with liver cirrhosis who experienced worsening of his ascites, edemas of the GB and intestinal wall and spleen enlargement after balloon-occluded retrograde transvenous obliteration. The serum albumin levels before and after balloonoccluded retrograde transvenous obliteration were 2.3 g/dL and 2.0 g/dL, respectively. A, B. The pre- (A) and post-procedural (B) CT scans at the level of the dome of the liver, obtained 20 hours before balloon-occluded retrograde transvenous obliteration and 66 hours after balloon-occluded retrograde transvenous obliteration, respectively, show the new development of ascites (arrow). His total ascites score increased from zero to 6 after balloon-occluded retrograde transvenous obliteration. C, D. The pre- (C) and post-procedural (D) CT scans at the GB level show the new development of GB edema after balloon-occluded retrograde transvenous obliteration (arrows), in which the maximum GB wall thickness increased from 2 mm to 5 mm. E, F. The pre- (E) and post-procedural (F) CT scans at the level of the right renal hilum show the new development of intestinal wall edema involving the ascending, transverse and descending colon (arrows).
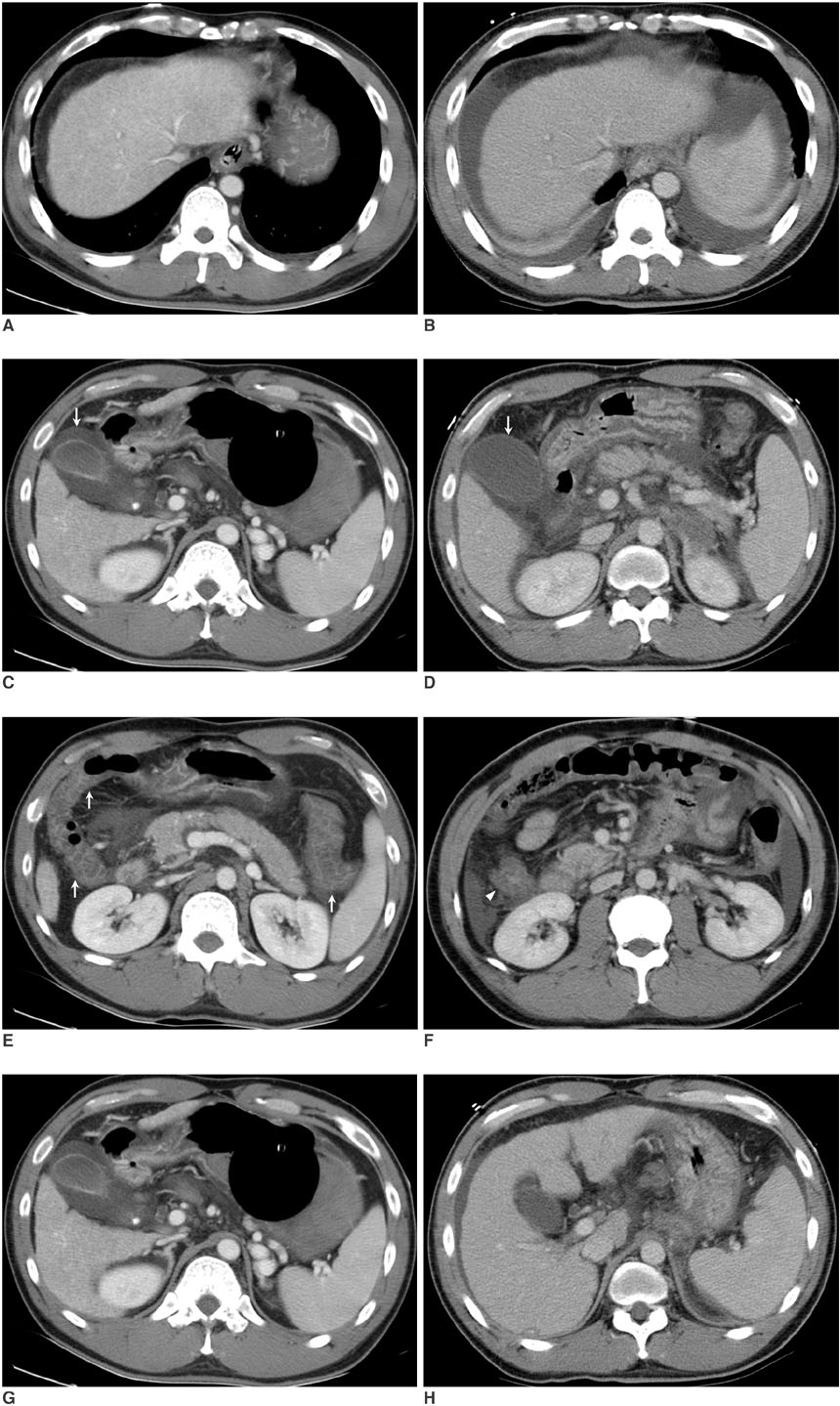
Fig. 2 Patient 2. A 37-old-year man with liver cirrhosis who experienced the development of ascites and spleen enlargement, but also improvement of his intestinal wall edema and his GB edema disappeared after balloon-occluded retrograde transvenous obliteration. The serum albumin levels before and after balloon-occluded retrograde transvenous obliteration were 2.2 g/dL and 2.8 g/dL, respectively. A, B. Pre- (A) and post-procedural (B) CT scans at the level of the dome of the liver, obtained 18 hours before balloon-occluded retrograde transvenous obliteration and 51 hours after balloon-occluded retrograde transvenous obliteration, respectively, show the development of new bilateral ascites. His total ascites score increased from zero to 8 after balloon-occluded retrograde transvenous obliteration. C, D. The pre- (C) and post-procedural (D) CT scans at the GB level show that the GB edema has disappeared after balloon-occluded retrograde transvenous obliteration (arrows), and there is a reduction in the maximum GB wall thickness from 10 mm to 2 mm. E, F. Diffuse bowel wall thickening (> 6 mm) is evident in the ascending, transverse, and descending colon (arrows) on the pre-procedural CT scans (E), but this is seen only in the ascending colon (arrowhead) on the post-procedural CT scans (F), which indicates that the intestinal wall edema is much improved after balloon-occluded retrograde transvenous obliteration. G, H. The pre- (G) and post-procedural (H) CT scans at the splenic hilum level show splenic enlargement after balloon-occluded retrograde transvenous obliteration. A volume calculation indicated a 120% increase of the spleen volume.
Cited by 1 articles
-
The Role of Divided Injections of a Sclerotic Agent over Two Days in Balloon-Occluded Retrograde Transvenous Obliteration for Large Gastric Varices
Takuji Yamagami, Rika Yoshimatsu, Hiroshi Miura, Tomohiro Matsumoto, Terumitsu Hasebe
Korean J Radiol. 2013;14(3):439-445. doi: 10.3348/kjr.2013.14.3.439.
Reference
-
1. Sugimori K, Morimoto M, Shirato K, Kokawa A, Tomita N, Numata K, et al. Retrograde transvenous obliteration of gastric varices associated with large collateral veins or a large gastrorenal shunt. J Vasc Interv Radiol. 2005. 16:113–118.2. Ninoi T, Nakamura K, Kaminou T, Nishida N, Sakai Y, Kitayama T, et al. TIPS versus transcatheter sclerotherapy for gastric varices. AJR Am J Roentgenol. 2004. 183:369–376.3. Choi YH, Yoon CJ, Park JH, Chung JW, Kwon JW, Choi GM. Balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding: its feasibility compared with transjugular intrahepatic portosystemic shunt. Korean J Radiol. 2003. 4:109–116.4. Kitamoto M, Imamura M, Kamada K, Aikata H, Kawakami Y, Matsumoto A, et al. Balloon-occluded retrograde transvenous obliteration of gastric fundal varices with hemorrhage. AJR Am J Roentgenol. 2002. 178:1167–1174.5. Koito K, Namieno T, Nagakawa T, Morita K. Balloon-occluded retrograde transvenous obliteration for gastric varices with gastrorenal or gastrocaval collaterals. AJR Am J Roentgenol. 1996. 167:1317–1320.6. Hirota S, Matsumoto S, Tomita M, Sako M, Kono M. Retrograde transvenous obliteration of gastric varices. Radiology. 1999. 211:349–356.7. Arai H, Abe T, Shimoda R, Takagi H, Yamada T, Mori M. Emergency balloon-occluded retrograde transvenous obliteration for gastric varices. J Gastroenterol. 2005. 40:964–971.8. Chikamori F, Kuniyoshi N, Shibuya S, Takase Y. Eight years of experience with transjugular retrograde obliteration for gastric varices with gastrorenal shunts. Surgery. 2001. 129:414–420.9. Fukuda T, Hirota S, Sugimura K. Long-term results of balloon-occluded retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy. J Vasc Interv Radiol. 2001. 12:327–336.10. Nishida N, Ninoi T, Kitayama T, Tokunaga M, Sakai Y, Hamuro M, et al. Selective balloon-occluded retrograde transvenous obliteration of gastric varix with preservation of major portacaval shunt. AJR Am J Roentgenol. 2006. 186:1155–1157.11. Ninoi T, Nishida N, Kaminou T, Sakai Y, Kitayama T, Hamuro M, et al. Balloon-occluded retrograde transvenous obliteration of gastric varices with gastrorenal shunt: long-term follow-up in 78 patients. AJR Am J Roentgenol. 2005. 184:1340–1346.12. Kanagawa H, Mima S, Kouyama H, Gotoh K, Uchida T, Okuda K. Treatment of gastric fundal varices by balloon-occluded retrograde transvenous obliteration. J Gastroenterol Hepatol. 1996. 11:51–58.13. Sonomura T, Sato M, Kishi K, Terada M, Shioyama Y, Kimura M, et al. Balloon-occluded retrograde transvenous obliteration for gastric varices: a feasibility study. Cardiovasc Intervent Radiol. 1998. 21:27–30.14. Chikamori F, Kuniyoshi N, Shibuya S, Takase Y. Short-term hemodynamic effects of transjugular retrograde obliteration of gastric varices with gastrorenal shunt. Dig Surg. 2000. 17:332–336.15. Miyamoto Y, Oho K, Kumamoto M, Toyonaga A, Sata M. Balloon-occluded retrograde transvenous obliteration improves liver function in patients with cirrhosis and portal hypertension. J Gastroenterol Hepatol. 2003. 18:934–942.16. Akahane T, Iwasaki T, Kobayashi N, Tanabe N, Takahashi N, Gama H, et al. Changes in liver function parameters after occlusion of gastrorenal shunts with balloon-occluded retrograde transvenous obliteration. Am J Gastroenterol. 1997. 92:1026–1030.17. Cardoso JE, Gautreau C, Jeyaraj PR, Patrzalek D, Cherruau B, Vaubourdolle M, et al. Augmentation of portal blood flow improves function of human cirrhotic liver. Hepatology. 1994. 19:375–380.18. Kiyosue H, Mori H, Matsumoto S, Yamada Y, Hori Y, Okino Y. Transcatheter obliteration of gastric varices: Part 2. Strategy and techniques based on hemodynamic features. Radiographics. 2003. 23:921–937. discussion 937.19. Breiman RS, Beck JW, Korobkin M, Glenny R, Akwari OE, Heaston DK, et al. Volume determinations using computed tomography. AJR Am J Roentgenol. 1982. 138:329–333.20. Henderson JM, Heymsfield SB, Horowitz J, Kutner MH. Measurement of liver and spleen volume by computed tomography. Assessment of reproducibility and changes found following a selective distal splenorenal shunt. Radiology. 1981. 141:525–527.21. Shen S, DeNardo GL, Yuan A, Hartmann-Siantar C, O'Donnell RT, DeNardo SJ. Splenic volume change and nodal tumor response in non-Hodgkin's lymphoma patients after radioimmunotherapy using radiolabeled Lym-1 antibody. Cancer Biother Radiopharm. 2005. 20:662–670.22. Ito K, Higuchi M, Kada T, Mitchell DG, Nomura S, Honjo K, et al. CT of acquired abnormalities of the portal venous system. Radiographics. 1997. 17:897–917.23. Cho KC, Patel YD, Wachsberg RH, Seeff J. Varices in portal hypertension: evaluation with CT. Radiographics. 1995. 15:609–622.24. Wang TF, Hwang SJ, Lee EY, Tsai YT, Lin HC, Li CP, et al. Gall-bladder wall thickening in patients with liver cirrhosis. J Gastroenterol Hepatol. 1997. 12:445–449.25. Saverymuttu SH, Grammatopoulos A, Meanock CI, Maxwell JD, Joseph AE. Gallbladder wall thickening (congestive cholecystopathy) in chronic liver disease: a sign of portal hypertension. Br J Radiol. 1990. 63:922–925.26. Baba Y, Hokotate H, Inoue H, Nakajo M. Correlations between colonic wall thickening in patients with virally induced cirrhosis on CT and clinical status. J Comput Assist Tomogr. 2001. 25:786–791.27. Guingrich JA, Kuhlman JE. Colonic wall thickening in patients with cirrhosis: CT findings and clinical implications. AJR Am J Roentgenol. 1999. 172:919–924.28. Chikamori F, Kuniyoshi N, Shibuya S, Takase Y. Transjugular retrograde obliteration for chronic portosystemic encephalopathy. Abdom Imaging. 2000. 25:567–571.29. Shimoda R, Horiuchi K, Hagiwara S, Suzuki H, Yamazaki Y, Kosone T, et al. Short-term complications of retrograde transvenous obliteration of gastric varices in patients with portal hypertension: effects of obliteration of major portosystemic shunts. Abdom Imaging. 2005. 30:306–313.30. Fukuda T, Hirota S, Matsumoto S, Sugimoto K, Fujii M, Tsurusaki M, et al. Application of balloon-occluded retrograde transvenous obliteration to gastric varices complicating refractory ascites. Cardiovasc Intervent Radiol. 2004. 27:64–67.31. Bezerra AS, D'Ippolito G, Faintuch S, Szejnfeld J, Ahmed M. Determination of splenomegaly by CT: is there a place for a single measurement? AJR Am J Roentgenol. 2005. 184:1510–1513.32. Prassopoulos P, Daskalogiannaki M, Raissaki M, Hatjidakis A, Gourtsoyiannis N. Determination of normal splenic volume on computed tomography in relation to age, gender and body habitus. Eur Radiol. 1997. 7:246–248.33. Spencer RP, Pearson HA. The spleen as a hematological organ. Semin Nucl Med. 1975. 5:95–102.34. Ralls PW, Quinn MF, Juttner HU, Halls JM, Boswell WD. Gallbladder wall thickening: patients without intrinsic gallbladder disease. AJR Am J Roentgenol. 1981. 137:65–68.35. Balthazar EJ, Gade MF. Gastrointestinal edema in cirrhotics. Radiographic manifestations and pathogenesis with emphasis on colonic involvement. Gastrointest Radiol. 1976. 1:215–223.36. Kozarek RA, Botoman VA, Bredfeldt JE, Roach JM, Patterson DJ, Ball TJ. Portal colopathy: prospective study of colonoscopy in patients with portal hypertension. Gastroenterology. 1991. 101:1192–1197.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Balloon Occluded Retrograde Transvenous Obliteration of Bleeding Stomal Varices Using Sodium Tetradecyl Sulfate Foam: A Case Report
- Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varix with Both Gastrorenal and Gastrocaval Shunts: A Case Report
- Balloon-occluded retrograde transvenous obliteration for bleeding gastric varices in a patient without a gastrorenal shunt
- Comparison of Coil Embolization and Slcerotherapy of Collateral Veins during Balloon Occluded Retrograde Transvenous Obliteration: Its Long Term Effect for Gastric Varix Treatment
- Balloon Occlusion Retrograde Transvenous Obliteration of Gastric Varices in Two Non-Cirrhotic Patients with Portal Vein Thrombosis
