The Sentinel Clot Sign: a Useful CT Finding for the Evaluation of Intraperitoneal Bladder Rupture Following Blunt Trauma
- Affiliations
-
- 1Department of Radiology, Chonnam National University Medical School, Gwangju, Korea. kjradsss@dreamwiz.com
- 2Department of Urology, Chonnam National University Medical School, Gwangju, Korea.
- 3Clinical Trial Center, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 1089436
- DOI: http://doi.org/10.3348/kjr.2007.8.6.492
Abstract
- OBJECTIVE: To evaluate the frequency and relevance of the "sentinel clot" sign on CT for patients with traumatic intraperitoneal bladder rupture in a retrospective study. MATERIALS AND METHODS: During a recent 42-month period, 74 consecutive trauma patients (45 men, 29 women; age range, 12-84 years; mean age, 50.8 years) with gross hematuria were examined by the use of intravenous contrast-enhanced CT of the abdomen and pelvis, followed by retrograde cystography. Contrast-enhanced CT scanning was performed by using a helical CT scanner. CT images were retrospectively reviewed in consensus by two radiologists. The CT findings including the sentinel clot sign, pelvic fracture, traumatic injury to other abdominal viscera, and the degree of intraperitoneal free fluid were assessed and statistically analyzed using the two-tailed x2 test. RESULTS: Twenty of the 74 patients had intraperitoneal bladder rupture. The sentinel clot sign was seen for 16 patients (80%) with intraperitoneal bladder rupture and for four patients (7%) without intraperitoneal bladder rupture (p < 0.001). Pelvic fracture was noted in five patients (25%) with intraperitoneal bladder rupture and in 39 patients (72%) without intraperitoneal bladder rupture (p < 0.001). Intraperitoneal free fluid was found in all patients (100%) with intraperitoneal bladder rupture, irrespective of an associated intraabdominal visceral injury, whereas 19 (35%) of the 54 patients without intraperitoneal bladder rupture had intraperitoneal free fluid (p < 0.001). CONCLUSION: Detection and localization of the sentinel clot sign abutting on the bladder dome may improve the accuracy of CT in the diagnosis of traumatic intraperitoneal bladder rupture, especially when the patients present with gross hematuria.
Keyword
MeSH Terms
-
Abdominal Injuries/diagnosis/etiology
Adolescent
Adult
Aged
Aged, 80 and over
Child
Contrast Media/administration & dosage
Extravasation of Diagnostic and Therapeutic Materials/diagnosis/etiology
Female
Fractures, Bone/diagnosis/etiology
Hematuria/etiology
Humans
Image Processing, Computer-Assisted
Iohexol/diagnostic use
Male
Middle Aged
Observer Variation
Pelvic Bones/injuries/radiography
Predictive Value of Tests
Radiographic Image Enhancement/methods
Reproducibility of Results
Retrospective Studies
Rupture/diagnosis
Tomography, Spiral Computed/*methods
Urinary Bladder/*injuries/*radiography
Wounds, Nonpenetrating/complications/*diagnosis
Figure
-

Fig. 1 An 84-year-old man with an intraperitoneal bladder rupture. A. A transverse unenhanced CT image shows a high-attenuating hematoma (arrows) with an attenuation of 57 HU abutting on the bladder dome filled with low-attenuating fluid (arrowheads). B. A coronal reformatted CT image clearly depicts a high-attenuating hematoma (arrows) on the bladder. C. A conventional cystogram obtained with the patient in the supine position shows extravasation of contrast material into the intraperitoneal space.
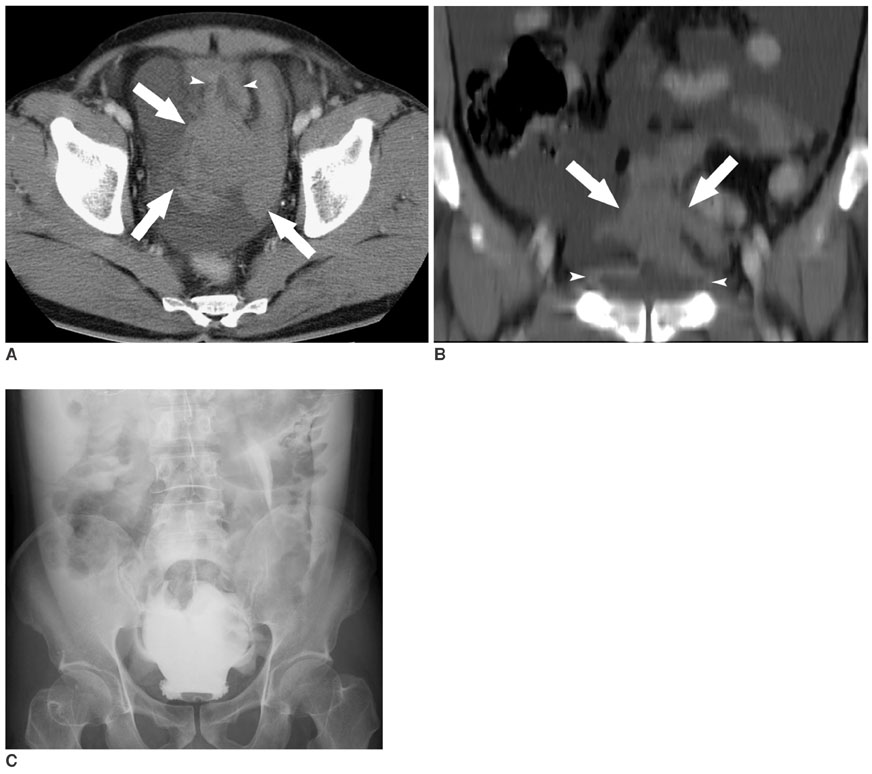
Fig. 2 A 51-year-old man with an intraperitoneal bladder rupture. A. A transverse contrast-enhanced CT image shows a high-attenuating hematoma (arrows) with an attenuation of 59 HU abutting on the collapsed bladder dome (arrowheads). B. A coronal reformatted CT image clearly depicts a high-attenuating hematoma (arrows) on the bladder (arrowheads). C. A conventional cystogram obtained with the patient in the supine position shows extravasation of contrast material into the intraperitoneal space.
Reference
-
1. Morey AF, Iverson AJ, Swan A, Harmon WJ, Spore SS, Bhayani S, et al. Bladder rupture after blunt trauma: guidelines for diagnostic imaging. J Trauma. 2001. 51:683–686.2. Vaccaro JP, Brody JM. CT cystography in the evaluation of major bladder trauma. RadioGraphics. 2000. 20:1373–1381.3. Power N, Ryan S, Hamilton P. Computed tomographic cystography in bladder trauma: pictorial essay. Can Assoc Radiol J. 2004. 55:304–308.4. Corriere JN Jr, Sandler CM. Diagnosis and management of bladder injuries. Urol Clin North Am. 2006. 33:67–71.5. Peng MY, Parisky YR, Cornwell EE 3rd, Radin R, Bragin S. CT cystography versus conventional cystography in evaluation of bladder injury. AJR Am J Roentgenol. 1999. 173:1269–1272.6. Kane NM, Francis IR, Ellis JH. The values of CT in the detection of bladder and posterior urethral injuries. AJR Am J Roentgenol. 1989. 153:1243–1246.7. Haas CA, Brown SL, Spirnak JP. Limitations of routine spiral computerized tomography in the evaluation of bladder trauma. J Urol. 1999. 162:51–52.8. Pao DM, Ellis JH, Cohan RH, Korobkin M. Utility of routine trauma CT in the detection of bladder rupture. Acad Radiol. 2000. 7:317–324.9. Orwig D, Federle MP. Localized clotted blood as evidence of visceral trauma on CT: the sentinel clot sign. AJR Am J Roentgenol. 1989. 153:747–749.10. Federle MP, Jeffrey RB. Hemoperitoneum studied by computed tomography. Radiology. 1983. 148:187–192.11. Sandler CM, Hall JT, Rodriguez MB, Corriere JN. Bladder injury in blunt pelvic trauma. Radiology. 1986. 158:633–638.12. Wah TM, Spencer JA. The role of CT in the management of adult urinary tract trauma. Clin Radiol. 2001. 56:268–277.13. Gomez RG, Ceballos L, Coburn M, Corriere JN Jr, Dixon CM, Lobel B, et al. Consensus statement on bladder injuries. BJU Int. 2004. 94:27–32.14. Brandes S, Borrelli J Jr. Pelvic fracture and associated urologic injuries. World J Surg. 2001. 25:1578–1587.15. Morgan DE, Nallamala LK, Kenney PJ, Mayo MS, Rue LW 3rd. CT cystography: radiographic and clinical predictors of bladder rupture. AJR Am J Roentgenol. 2000. 174:89–95.16. Rodriguez C, Barone JE, Wilbanks TO, Rha CK, Miller K. Isolated free fluid on computed tompgraphic scan in blunt abdominal trauma: a systematic review of incidence and management. J Trauma. 2002. 53:79–85.17. Ng AK, Simons RK, Torreggiani WC, Ho SG, Kirkpatrick AW, Brown DR. Intra-abdominal free fluid without solid organ injury in blunt abdominal trauma: an indication for laparotomy. J Trauma. 2002. 52:1134–1140.18. Cunningham MA, Tyroch AH, Kaups KL, Davis JW. Does free fluid on abdominal computed tomographic scan after blunt trauma require laparotomy? J Trauma. 1998. 44:599–603.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation of Bladder Rupture due to Blunt Trauma
- A Case of Neobladder Rupture Following Blunt Trauma
- Vesical and paravesical injuries: CT findings
- The Role of Computerized Tomography in the Diagnosis of Bladder Rapture
- Laparoscopic Repair of Traumatic Intraperitoneal Bladder Rupture: A Case Series
