Diffuse Interstitial Infiltrative Lung Metastasis of Malignant Melanoma: a Case Report
- Affiliations
-
- 1Department of Radiology, Severance Hospital, Yonsei University School of Medicine, Seoul 120-752, Korea. iamotwo@yuhs.ac
- 2Department of Pathology, Severance Hospital, Yonsei University School of Medicine, Seoul 120-752, Korea.
- KMID: 1088572
- DOI: http://doi.org/10.3348/kjr.2011.12.2.252
Abstract
- A diffuse interstitial infiltrative pattern of lung metastasis in a patient with malignant melanoma is rare and can be confused with benign conditions such as pulmonary edema or drug-induced pneumonitis. We experienced a case of diffuse interstitial infiltrative lung metastasis in malignant melanoma in a 37-year-old man. This case was confirmed by a transbronchial lung biopsy. We herein describe the findings on CT and positron emission tomography scan.
Keyword
MeSH Terms
Figure
-
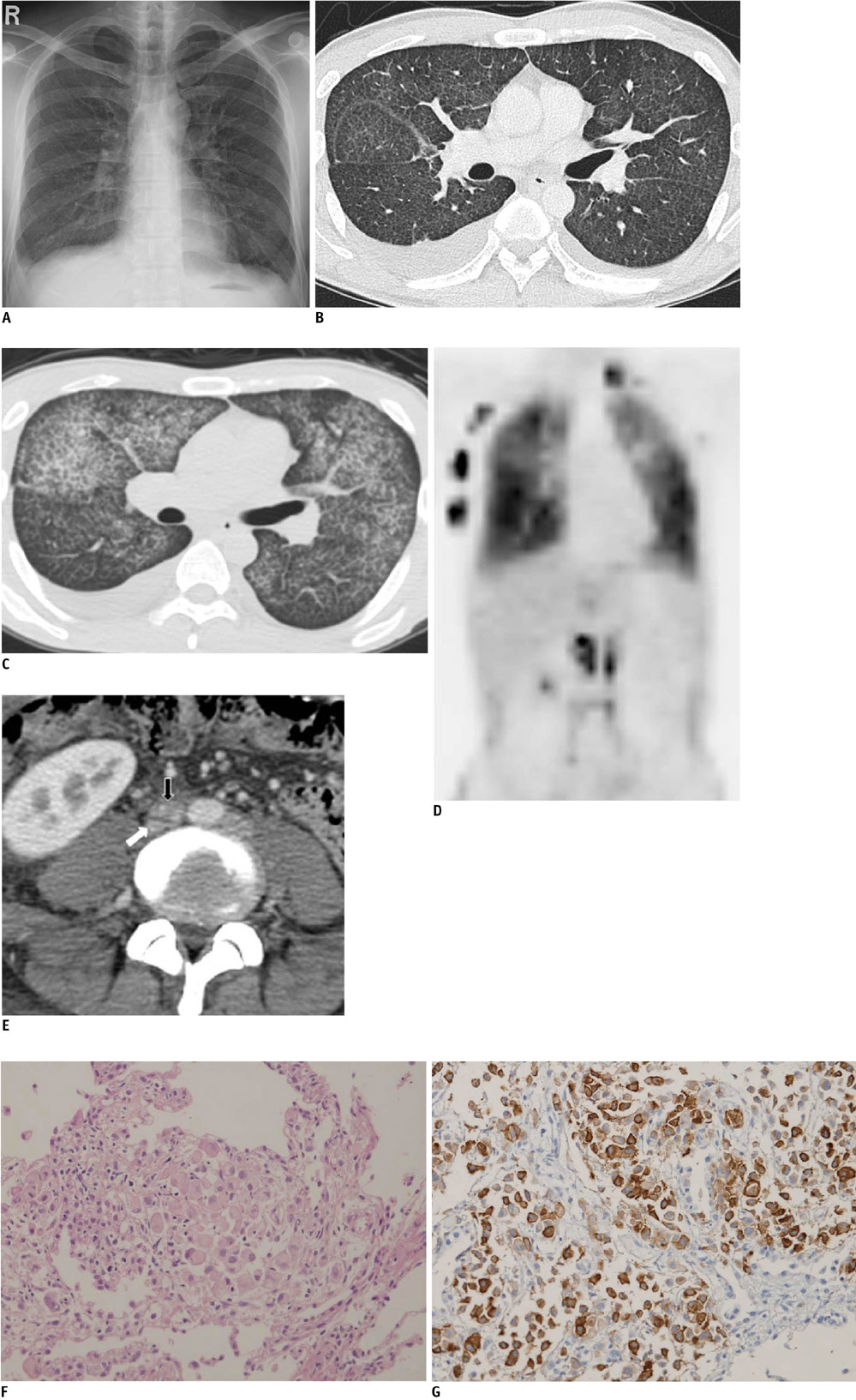
Fig. 1 38-year-old man with diffuse interstitial infiltrative lung metastasis of malignont melanoma. A. Chest radiograph shows diffuse reticulonodular opacities in both of lungs with bilateral pleural effusions. B. Chest CT image (lung window) demonstrates intralobular interstitial thickenings and areas of ground-glass opacity with bilateral pleural effusions. C-E. Follow-up FDG PET/CT scan two months later shows extensive intralobular interstitial thickenings and diffuse areas of ground-glass opacity with bilateral pleural effusions on contrast-enhanced CT image (lung window) (C) and diffusely increased FDG uptake in both lungs with metastatic LNs in right chest wall, left neck, and retroperitoneum on PET image (D) CT image shows irregular narrowing of inferior vena cava (white arrow), suggesting invasion of inferior vena cava by metastatic aortocaval lymph node (black arrow) (E). F. Photomicrographs of histologic specimens show that tumor cells predominantly infiltrates in alveolar capillaries and interstitium. Tumor cells are round to oval in shape with enlarged nuclei and plump cytoplasm. G. Immunohistochemical stain for HMB-45 is positive for tumor cells.
Reference
-
1. Lee YT. Malignant melanoma: pattern of metastasis. CA Cancer J Clin. 1980. 30:137–142.2. Webb WR, Gamsu G. Thoracic metastasis in malignant melanoma. A radiographic survey of 65 patients. Chest. 1977. 71:176–181.3. Dwyer AJ, Reichert CM, Woltering EA, Flye MW. Diffuse pulmonary metastasis in melanoma: radiographic-pathologic correlation. AJR Am J Roentgenol. 1984. 143:983–984.4. Chen JT, Dahmash NS, Ravin CE, Heaston DK, Putman CE, Seigler HF, et al. Metastatic melanoma in the thorax: report of 130 patients. AJR Am J Roentgenol. 1981. 137:293–298.5. Akira M, Ishikawa H, Yamamoto S. Drug-induced pneumonitis: thin-section CT findings in 60 patients. Radiology. 2002. 224:852–860.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- DILD (diffuse infiltrative lung disease); Radiologic Diagnostic Approach According to High-Resolution CT Pattern
- Diagnosis and management of primary malignant melanoma of the lung: a case report
- A Case of Unknown Primary Malignant Melanoma with Pulmonary and Endobronchial Metastasis
- Surgical Resection of Metastatic Choroidal Melanoma in the Rib and Bronchus: A case report
- Esophageal Metastasis of Malignant Melanoma in a 66-year-old Female Patient
