Various Tumor-Mimicking Lesions in the Musculoskeletal System: Causes and Diagnostic Approach
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Medical Center, Seoul 130-702, Korea. gdluck@hitel.net
- 2Department of Radiology, East-West Neo Medical Center, Kyung Hee University, Seoul 134-727, Korea.
- KMID: 1088568
- DOI: http://doi.org/10.3348/kjr.2011.12.2.220
Abstract
- Tumor-mimicking lesions in the musculoskeletal system can be defined as lesions mistaken as tumors due to the presence of palpation upon physical examination or a tumor-like appearance upon radiological examination. Moreover, tumor-mimicking lesions show diverse etiologies and anatomic locations. We illustrated the various tumor-mimicking lesions involving bone and soft tissue. In this review, the tumor-mimicking lesions were classified into those based on clinical examination and those based on radiological examination in musculoskeletal radiology. Awareness of the various causes of tumor-mimicking lesions, correctly obtaining clinical information, and the proper selection of imaging modality are important for the differentiation of tumor-mimicking lesions from true neoplasms.
Keyword
MeSH Terms
Figure
-
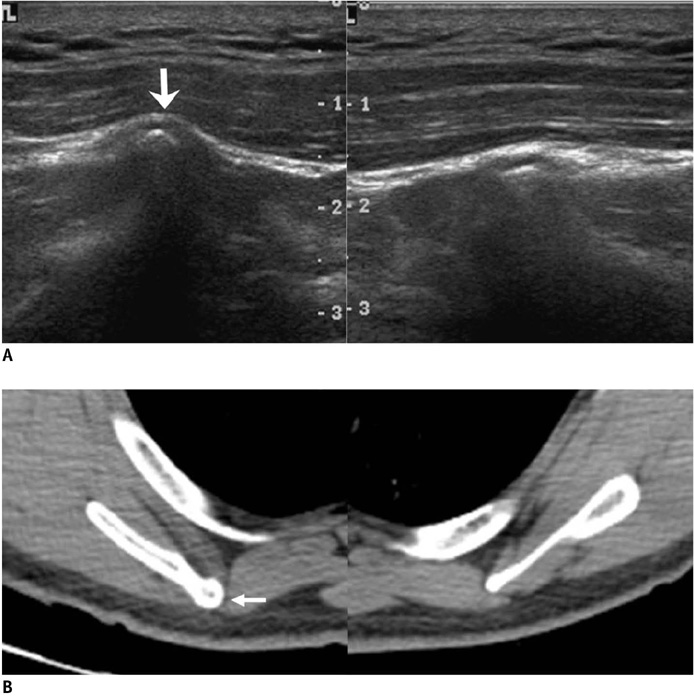
Fig. 1 51-year-old male with right back mass. A. Transverse sonograms of both scapulas show protruding medial inferior border of right scapula (arrow). B. On axial CT image, right scapula reveals larger size, more superficial location of medial inferior border (arrow), and different course compared to those of contralateral side.
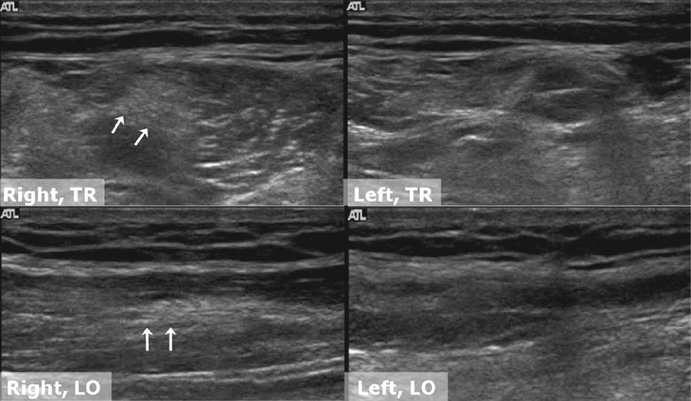
Fig. 2 49-year-old male with painful mass in posterior aspect of right thigh. Transverse and longitudinal sonograms reveal thickened musculotendinous transition zone of right semitendinosus muscle tendon (arrows) compared to that of contralateral side.
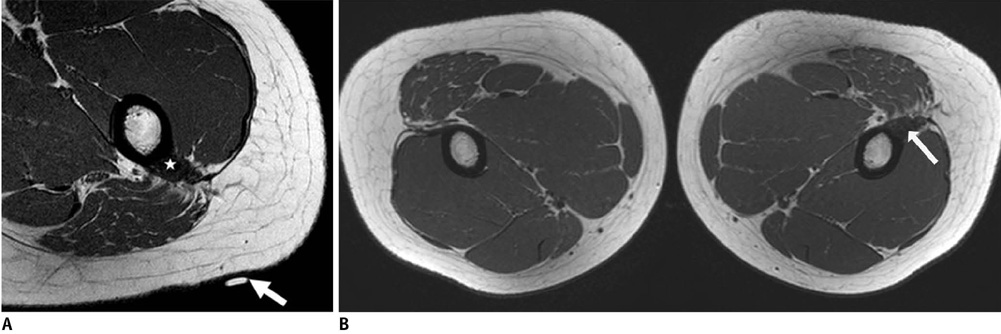
Fig. 3 18-year-old female with palpable lesion on left buttock. A. There is no space-occupying lesion or signal abnormality near marker (arrow) indicating palpable site, but thickened gluteus maximus tendon at femoral attachment site (star) with slight fatty atrophy of gluteus maximus muscle and depressed groove is noted on axial T1-weighted image. B. Additional axial T1-weighted image of both hips demonstrates prominent thickening of left gluteus maximus tendon (arrow) compared to right side, possibly related to contracture of gluteus muscle.

Fig. 4 31-year-old male with palpable mass in left shoulder. T1-weighted coronal image demonstrates hypertrophy of left trapezius and supraspinatus muscles. Differential diagnosis includes cervical dystonia and accessory nerve injury.

Fig. 5 24-year-old male with focal enlargement of right buttock. A. Sonograms depict focal increased thickness of subcutaneous fat layer of right buttock (double-headed arrows) that can be compared with contralateral subcutaneous fat layer of left buttock. B. Axial T1-weighted image shows abundant fat deposition without signal change or mass effect in subcutaneous layer of right lateral buttock (arrows). Patient had recent history of rapid weight gain.
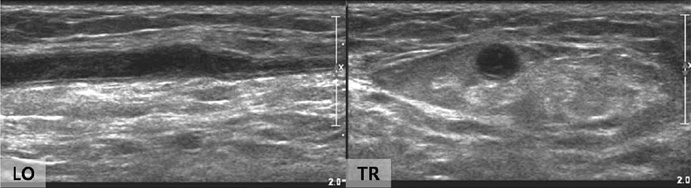
Fig. 6 78-year-old male with cord-like feeling in right forearm. Segmental obstruction with echogenic materials and dilation of basilic vein with wall thickening, is evident on longitudinal and transverse sonograms, suggesting superficial thrombophlebitis. Patient had history of intravenous catheterization in right forearm.
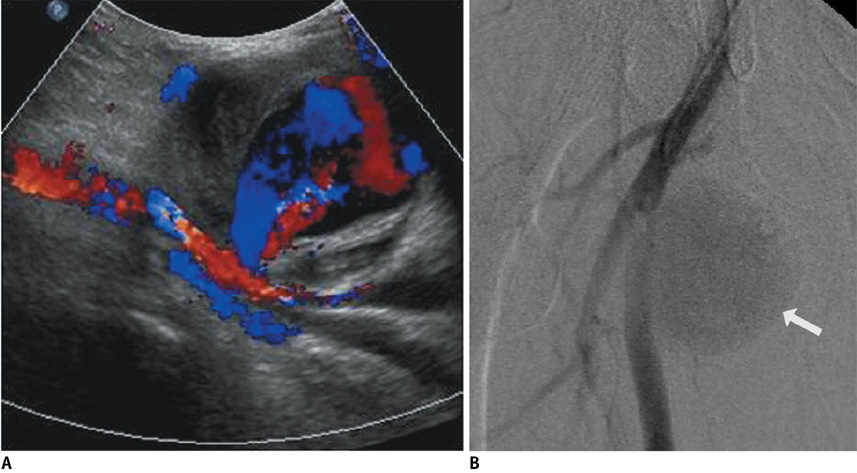
Fig. 7 65-year-old male with pulsating palpable mass in right inguinal region. A. Color Doppler sonogram shows blood flow in pseudoaneurysm cavity with characteristic swirling appearance and communicating channel with femoral artery at its base. B. Angiography reveals large pseudoaneurysm (arrow) in right superficial femoral artery.

Fig. 8 57-year-old male with painful nodule on lateral aspect of left thigh. A. Longitudinal sonogram shows calcified nodule with obvious acoustic shadowing in lateral aspect of proximal third of left femur. B. Radiograph of left femur shows round, homogeneous, cloud-like collection of calcifications at lateral aspect of left femur (arrow).

Fig. 9 66-year-old male with migrating palpable lesions in right thigh. Few well-defined, tortuous, lobulating, hypoechoic, tubular lesions in subcutaneous fat layer of right thigh are demonstrated on sonograms. Note thin linear hyperechogenicity (arrow) in hypoechoic portion of tubular lesions and surrounding vascularity. These were confirmed as sparganosis infestation.
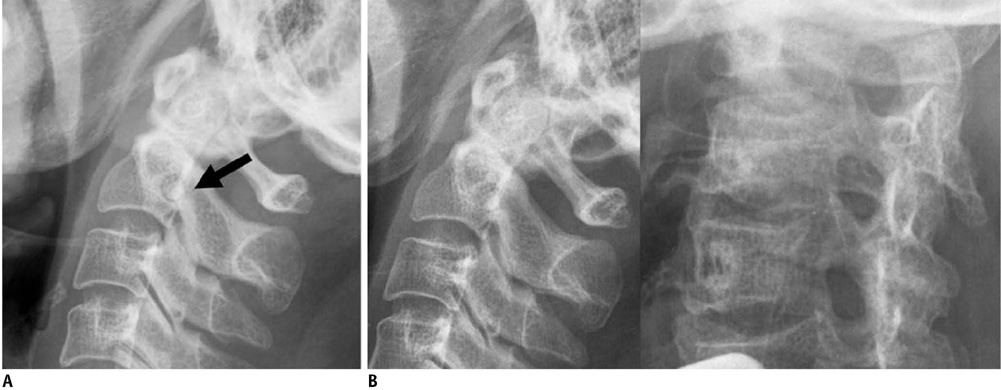
Fig. 10 54-year-old female with neck pain. A. Lateral view of cervical spine shows small, round sclerotic lesion with radiolucent rim (arrow) mimicking osteoid osteoma. B. As seen on follow-up lateral and right oblique views, there is no corresponding lesion in posterior element of C2. MRI confirmed that this was pseudolesion, which was thought to be superimposition of normal structures on lateral view.

Fig. 11 45-year-old male with history of scaphoid fracture. A. Ill-defined osteolytic lesion of distal radius (arrows) is depicted on plain radiograph. B. Axial CT scan reveals localized fat deposition in corresponding site on distal radius. Absence of capsule is feature that differentiates this from intraosseous lipoma.

Fig. 12 44-year-old hemophiliac with swelling of right thigh. A. Plain radiograph shows soft tissue mass with extrinsic bony erosion and periosteal reaction at right femur. B. Sagittal T2-weighted image demonstrates multilobular cystic lesion with dark-signal peripheral nodules, suggesting hemosiderin deposits. Diagnosis is intramuscular and subperiosteal hemophilic pseudotumor involving right thigh.

Fig. 13 38-year-old male with history of trauma. A. Coronal T2-weighted image shows marked heterogeneous lesion with high signal intensity in medial aspect of right thigh, resembling soft tissue sarcoma. B. Plain radiograph taken two months later demonstrates irregular calcification located along muscle on medial aspect of right thigh. Diagnosis was myositis ossificans.
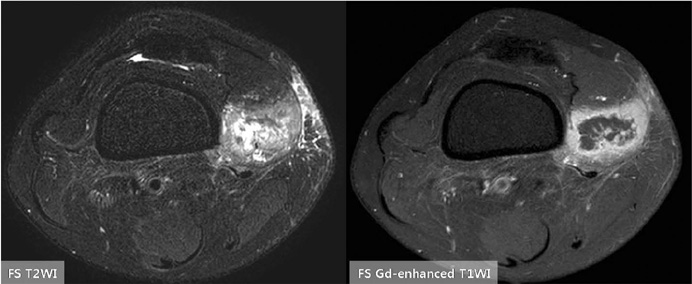
Fig. 14 39-year-old female with palpable mass in her medial thigh. Fat-suppressed axial T2-weighted image shows heterogeneous soft tissue mass located in distal part of right vastus medialis muscle, mimicking soft tissue sarcoma. Fat-suppressed enhanced T1-weighted image demonstrates mass with strong peripheral enhancement and central necrosis. This mass was histologically confirmed as proliferative myositis.

Fig. 15 61-year-old female with history of complete remission of acute leukemia. A. Multiple peripherally-enhancing nodular lesions involving thoracolumbar vertebrae are noted on fat-suppressed enhanced T1-weighted sagittal MR image, which mimic metastases. B. Portal phase of abdomen CT shows multiple low-attenuated lesions in liver and spleen, which were confirmed as candidial infection. Decompression of epidural mass at T10 was performed, and spinal lesions were also diagnosed as candidiasis.
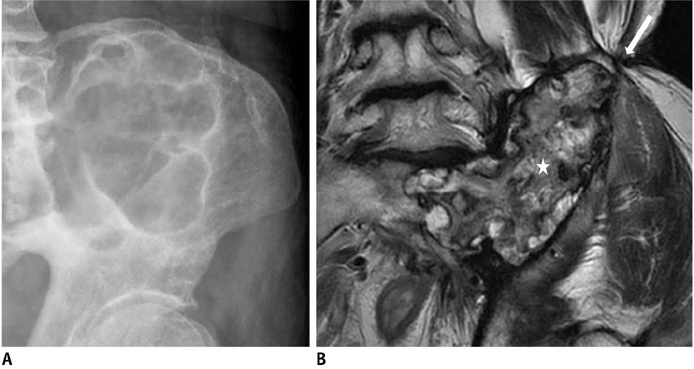
Fig. 16 47-year-old male with left hip pain. A. Plain radiograph demonstrates expansile, lobulating, osteolytic lesion in left ilium. Initial diagnosis was chondromyxoid fibroma. B. Coronal T2-weighted MR image shows extensive heterogeneous soft tissue mass (star) involving left ilium and sacrum with associated fistula (arrow), which was pathologically confirmed as chronic osteomyelitis.

Fig. 17 66-year-old female with complaints of right shoulder pain. A. Well-defined osteolytic lesion in right proximal humerus is noted on radiograph, suggesting benign tumor. B. Subperiosteal resorption is observed on phalanx. Parathyroid scan with Tc-99m MIBI, not shown, disclosed huge parathyroid mass. Therefore, osteolytic lesion was diagnosed as brown tumor caused by hyperparathyroidism.
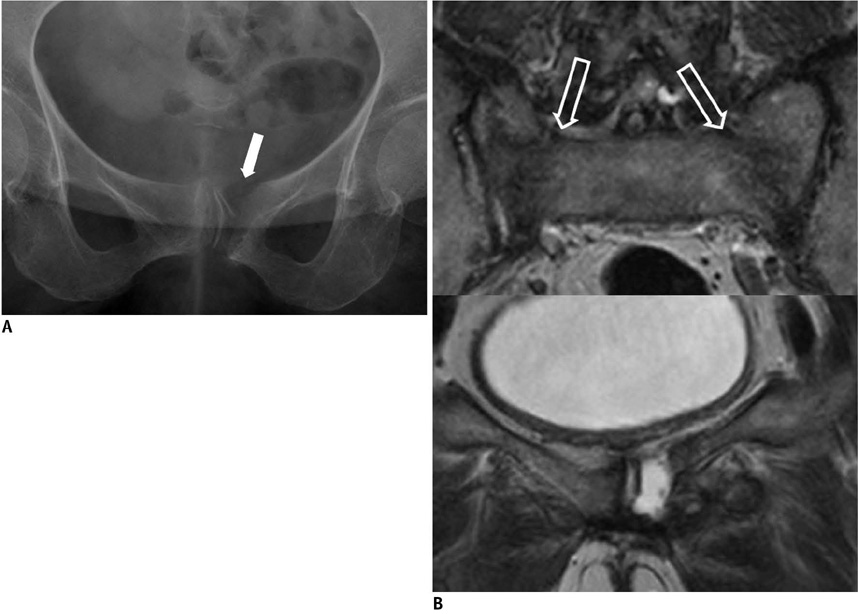
Fig. 18 63-year-old female with recent pain in pelvis. A. Plain radiograph of pelvis shows osteolytic lesion (arrow) of left pubic bone, mimicking metastasis. B. Two coronal T2-weighted images demonstrate fluid collection at left pubic bone, suggesting insufficiency fracture. Note another insufficiency fracture involving both sacral wings (open arrows).
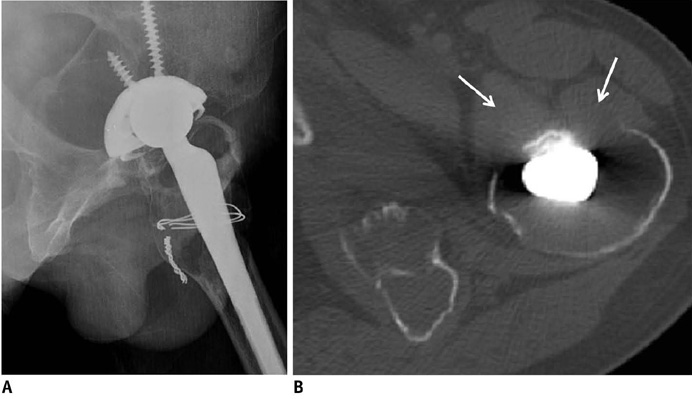
Fig. 19 37-year-old male with history of total hip replacement surgery 16 years ago. A. Plain radiograph shows well-defined, radiolucent lesions of both acetabular and femoral components. B. CT image reveals osteolysis with extraosseous soft tissue mass (arrows) via cortical discontinuity.
Reference
-
1. Vessal S, Rai SB. Accessory extensor carpi radialis brevis muscle, a pseudomass of the distal forearm: ultrasound and MR appearances - case report and literature review. Clin Radiol. 2006. 61:442–445.2. Mattle HP, Hess CW, Ludin HP, Mumenthaler M. Isolated muscle hypertrophy as a sign of radicular or peripheral nerve injury. J Neurol Neurosurg Psychiatry. 1991. 54:325–329.3. Polesuk BS, Helms CA. Hypertrophied palmaris longus muscle, a pseudomass of the forearm: MR appearance--case report and review of the literature. Radiology. 1998. 207:361–362.4. Anderson MW, Benedetti P, Walter J, Steinberg DR. MR appearance of the extensor digitorum manus brevis muscle: a pseudotumor of the hand. AJR Am J Roentgenol. 1995. 164:1477–1479.5. Capelastegui A, Astigarraga E, Fernandez-Canton G, Saralegui I, Larena JA, Merino A. Masses and pseudomasses of the hand and wrist: MR findings in 134 cases. Skeletal Radiol. 1999. 28:498–507.6. Kalbermatten DF, Kalbermatten NT, Hertel R. Cotton-induced pseudotumor of the femur. Skeletal Radiol. 2001. 30:415–417.7. Resnick D. Diagnosis of bone and joint disorders. 1995. 3rd ed. Philadelphia: Saunders.8. Mellado JM, Ramos A, Salvadó E, Camins A, Danús M, Saurí A. Accessory ossicles and sesamoid bones of the ankle and foot: imaging findings, clinical significance and differential diagnosis. Eur Radiol. 2003. 13:Suppl 6. L164–L177.9. Anderson SE, Johnston JO, Steinbach LS. Pseudotumors of the shoulder invited review. Eur J Radiol. 2008. 68:147–158.10. Useche JN, de Castro AM, Galvis GE, Mantilla RA, Ariza A. Use of US in the evaluation of patients with symptoms of deep venous thrombosis of the lower extremities. Radiographics. 2008. 28:1785–1797.11. Ramon FA, Degryse HR, De Schepper AM, Van Marck EA. Calcific tendinitis of the vastus lateralis muscle. A report of three cases. Skeletal Radiol. 1991. 20:21–23.12. Thiele RG, Schlesinger N. Diagnosis of gout by ultrasound. Rheumatology (Oxford). 2007. 46:1116–1121.13. Schwartzfarb EM, Hametti JM, Romanelli P, Ricotti C. Foreign body granuloma formation secondary to silicone injection. Dermatol Online J. 2008. 14:20.14. Catalano OA, Dal Pozzo F, Grifi DN, Menchi I, Rosenthal DI. Paraffinoma of the knee. Skeletal Radiol. 2003. 32:485–488.15. De Wilde V, De Maeseneer M, Lenchik L, Van Roy P, Beeckman P, Osteaux M. Normal osseous variants presenting as cystic or lucent areas on radiography and CT imaging: a pictorial overview. Eur J Radiol. 2004. 51:77–84.16. Hammond I, Sheikh A, Rasuli P, Souza CA. Vertebral pseudolesion on lateral chest radiograph. AJR Am J Roentgenol. 2008. 190:W240–W241.17. Kransdorf MJ, Meis JM. From the archives of the AFIP. Extraskeletal osseous and cartilaginous tumors of the extremities. Radiographics. 1993. 13:853–884.18. De Smet AA, Norris MA, Fisher DR. Magnetic resonance imaging of myositis ossificans: analysis of seven cases. Skeletal Radiol. 1992. 21:503–507.19. Kransdorf MJ, Meis JM, Jelinek JS. Myositis ossificans: MR appearance with radiologic-pathologic correlation. AJR Am J Roentgenol. 1991. 157:1243–1248.20. Gaeta M, Mazziotti S, Minutoli F, Genitori A, Toscano A, Rodolico C, et al. MR imaging findings of focal myositis: a pseudotumour that may mimic muscle neoplasm. Skeletal Radiol. 2009. 38:571–578.21. Kransdorf MJ, Temple HT, Sweet DE. Focal myositis. Skeletal Radiol. 1998. 27:283–287.22. Son JM, Jee WH, Jung CK, Kim SI, Ha KY. Aspergillus spondylitis involving the cervico-thoraco-lumbar spine in an immunocompromised patient: a case report. Korean J Radiol. 2007. 8:448–451.23. Urban BA, Fishman EK, Goldman SM, Scott WW Jr, Jones B, Humphrey RL, et al. CT evaluation of amyloidosis: spectrum of disease. Radiographics. 1993. 13:1295–1308.24. Park JS, Ryu KN, Hong HP, Park YK, Chun YS, Yoo MC. Focal osteolysis in total hip replacement: CT findings. Skeletal Radiol. 2004. 33:632–640.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Musculoskeletal Applications of Elastography: a Pictorial Essay of Our Initial Experience
- Incidental Musculoskeletal Lesions Detected on Abdominopelvic CT Scans: A Pictorial Essay
- Primary Extracranial Meningioma Mimicking Musculoskeletal Malignancy: A Case Report
- Clinical Situations in which Musculoskeletal Ultrasound is Helpful
- Usefulness of strain elastography of the musculoskeletal system
