Yonsei Med J.
2008 Apr;49(2):322-324. 10.3349/ymj.2008.49.2.322.
Acupuncture Induced Necrotizing Aortitis with Infected Pseudoaneurysm Formation
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Cardiovascular Center, Yonsei University College of Medicine, Seoul, Korea. dbricasa@ajou.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Ajou University School of Medicine, Suwon, Korea.
- KMID: 1084507
- DOI: http://doi.org/10.3349/ymj.2008.49.2.322
Abstract
- Necrotizing aortitis is a rare and life-threatening complication of local or generalized bacterial infections and most commonly affects the abdominal aorta. We described a case of a 79-year-old man with an acupuncture-induced bacterial aortitis associated with pseudoaneurysm formation causing near rupture. The patient underwent emergent explolapartomy, resection of the infected aorta, wide debridement of surrounding infected tissues, and extra-anatomic axillary to bifemoral graft bypass. The microbiologic examination revealed Escherichia coli and methicillin resistant Staphylococcus aureus (MRSA). Necrotizing aortitis is very serious and fatal disease, careful history taking as well as rapid diagnosis and urgent treatment are of critical importance.
Keyword
MeSH Terms
-
Acupuncture/*methods
Acupuncture Therapy/adverse effects
Aged
Aneurysm, False/microbiology/*pathology
Aortitis/etiology/microbiology/*pathology
Bacterial Infections/microbiology
Escherichia coli/isolation & purification
Humans
Male
Necrosis
Staphylococcus aureus/isolation & purification
Tomography, X-Ray Computed
Figure
-

Fig. 1 Preoperative abdominal CT showed infected aortic pseudoaneurysmm of 5 cm in diameter with periaortic gangrenous gas formation (white arrow).
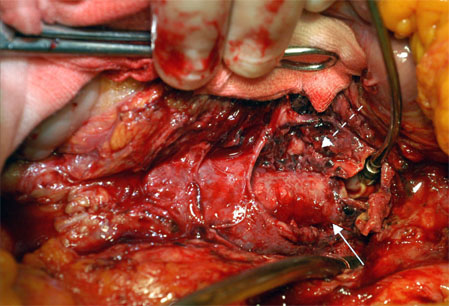
Fig. 2 Intraoperative finding revealed a pseudoaneurysm, containing gas-forming inflamed friable tissue with hematoma (dotted arrow), and the adventitia of the aorta wsa almost completely destroyed (solid arrow).
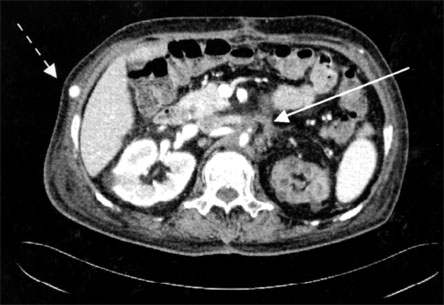
Fig. 3 Postoperative abdominal CT showed a 3 cm sized organizing fibrotic tissue around the area where the aorta was resected (solid arrow), and patent axillo-femoral prosthetic bypass graft (dotted arrow).
Reference
-
1. Lao L, Hamilton GR, Fu J, Berman BM. Is acupuncture safe? A systematic review of case reports. Altern Ther Health Med. 2003. 9:72–83.2. Foote EA, Postier RG, Greenfield RA, Bronze MS. Infectious Aortitis. Curr Treat Options Cardiovasc Med. 2005. 7:89–97.
Article3. Dawas K, Hicks RCJ. Pneumococcal aortitis causing aortic rupture. EJVES Extra. 2003. 6:70–72.
Article4. Luo CY, Ko WC, Kan CD, Lin PY, Yang YJ. In situ reconstruction of septic aortic pseudoaneurysm due to Salmonella or Streptococcus microbial aortitis: long-term follow-up. J Vasc Surg. 2003. 38:975–982.
Article5. Bronze MS, Shirwany A, Corbett C, Schaberg DR. Infectious aortitis: an uncommon manifestation of infection with Streptocuccus pneumoniae. Am J Med. 1999. 107:627–630.
Article6. Coppin T, Kassabian E, Costanzo A, Fabiani JN, Chemla E. Primary supraceliac aortic pseudoaneurysm due to a septic aortic rupture. J Cardiovasc Surg (Torino). 2005. 46:88–89.7. Kitamura T, Morota T, Motomura N, Ono M, Shibata K, Ueno K, et al. Management of infected grafts and aneurysms of the aorta. Ann Vasc Surg. 2005. 19:335–342.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tuberculous Aortitis Complicated with Pseudoaneurysm Formation in the Descending Thoracic Aorta: A Case Report
- Necrotizing Fasciitis of the Chest Wall Complicating Acupuncture
- Stanford Type A Aortic Dissection Secondary to Infectious Aortitis: A Case Report
- Iatrogenic or Traumatic Pseudoaneurysms of Peripheral Artery: 2 Cases Report
- A Case of Necrotizing Fasciitis of the Face
