An Effective Guidewire Looping Technique for the Recanalization of Occlusive Segments of Infrapopliteal Vessels
- Affiliations
-
- 1Institute of Diagnostic and Interventional Radiology, Shanghai Sixth People's Hospital, Shanghai Jiao Tong University, Shanghai 200233, China. zhao.jungong@163.com
- KMID: 984898
- DOI: http://doi.org/10.3348/kjr.2010.11.4.441
Abstract
OBJECTIVE
To determine the efficacy, safety and primary follow-up results of a guidewire looping technique for the treatment of infrapopliteal arteries.
MATERIALS AND METHODS
From October 2006 to May 2008, an intraluminal angioplasty of the infrapopliteal arteries was attempted in 200 consecutive patients. Altogether, 417 infrapopliteal lesions, with lengths varying from 2 cm to 32 cm, were treated as part of this study, including 305 lesions in the anterior tibial arteries, 89 in the posterior tibial arteries, and 23 in the peroneal arteries. The 'U'-shaped guidewire technique was attempted in 393 lesions from 361 limbs. The tip of a hydrophilic 0.035-inch guidewire was formed into a 'U' shape with the aid of a 4-Fr catheter and collateral branch vessel to recanalize the completely occluded long segment lesions.
RESULTS
A successful angioplasty with at least one artery recanalized directly to the malleolar or dorsal foot was achieved in 322 limbs (89%). The looping technique had a success rate of 90% (352 of 393 lesions). After the procedure, the rest pain was relieved in 58 of 69 patients, while 207 of 245 limbs (85%) showed improvement for intermittent claudication. Complete wound healing was noted in 21 of 54 patients, while 20 of 54 patients showed an improvement in the wound size or depth. A total of 38 major immediate procedure-related complications were noted, including retroperitoneal hematoma, distal emboli, and vessel rupture.
CONCLUSION
The results of this study suggests that the guidewire looping technique is a safe and effective method for the recanalization of the occluded lesions in infrapopliteal vessels.
MeSH Terms
Figure
-
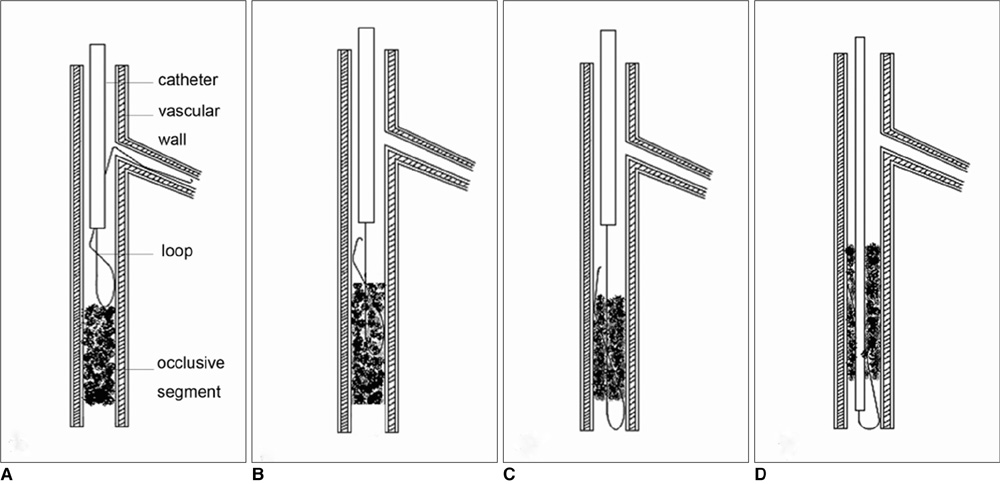
Fig. 1 Diagrams showing transluminal angioplasty technique. A. We first inserted hydrophilic guidewire into proximal branch and then made 'U' shape loop by rotating and advancing guidewire continually. B, C. Loop guidewire was advanced into and over occlusive segment of vessel. D. Catheter was crossed over occlusive segment along guidewire.
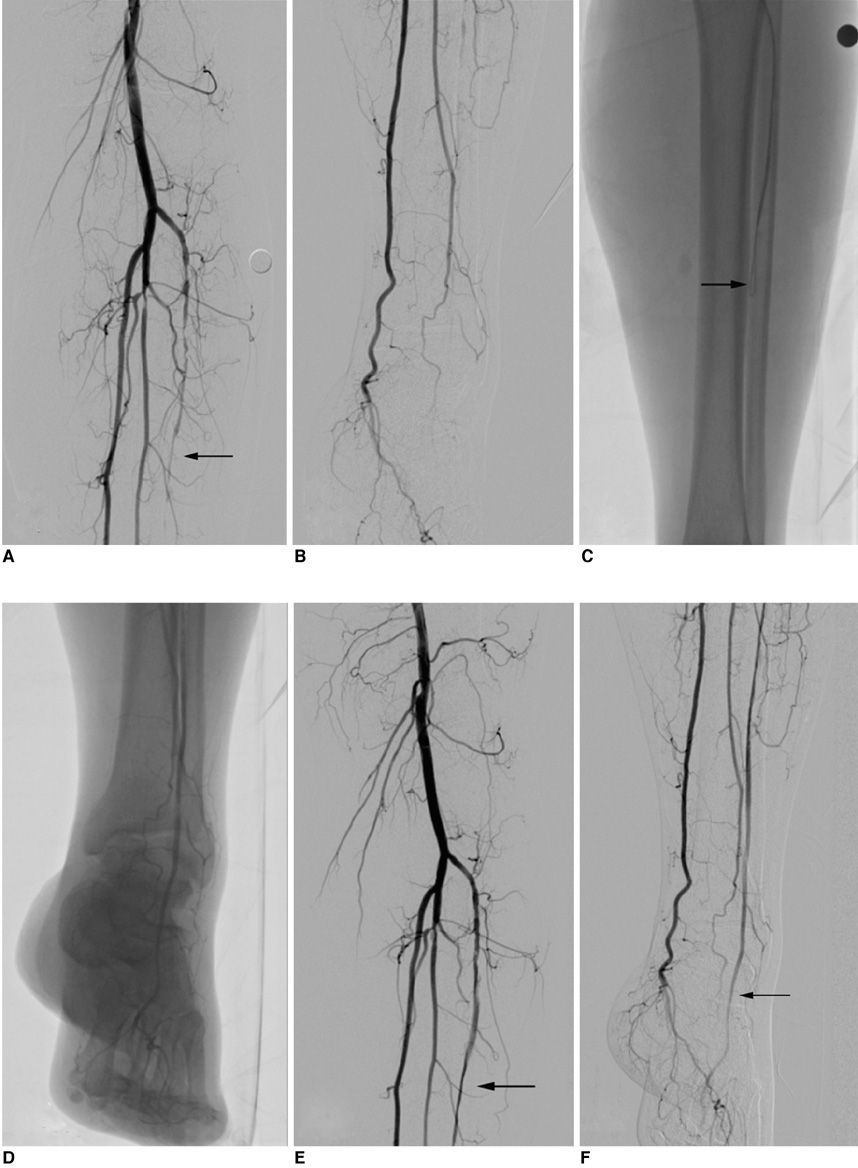
Fig. 2 67-year-old man with more than 10-year history of diabetes mellitus presented with symptoms of limb ischemia. A, B. Lateral lower limb angiogram revealed long segment of occlusive disease in anterior tibial artery along more than 15 cm, with faint run-off tract (arrow). C. Plain film showed head of hydrophilic guidewire (arrow) forming loop when passing through occlusive segment through 4-Fr vertebral catheter. D. Fluoroscopic angiogram demonstrated run-off tract indicating true lumen process. E, F. Immediate angiogram performed post-procedure showed restoration of anterior tibial artery with straight-line flow to pedal arch. Residual stenosis was less than 30% (arrows).
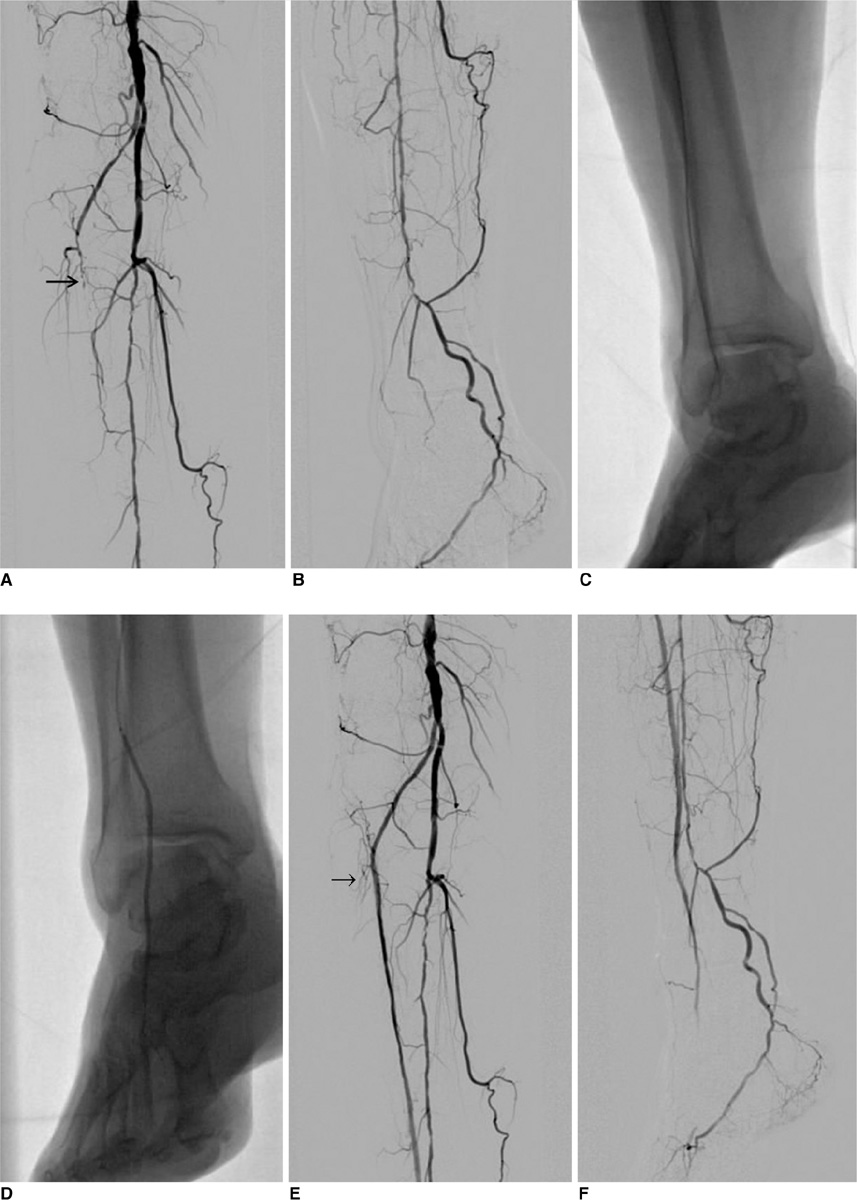
Fig. 3 69-year-old women with 15-year history of diabetes mellitus presented with gangrene in three to five toes of her right foot. A, B. Lateral lower limb angiograms reveals long segment of occlusive disease in anterior (arrow) and posterior tibial arteries. C, D. Plain films shows head of hydrophilic guidewire forming loop and passing through occluded segment with 4-Fr vertebral catheter and long balloon dilation of recanalized artery. E, F. Immediate angiograms performed post-procedure show restoration (arrow) of anterior tibial artery, but distal dorsal artery was embolized and subsequent thrombolysis did not work. Patient ultimately underwent below ankle amputation.
Reference
-
1. Dotter CT, Judkins MP. Transluminal treatment of arteriosclerotic obstruction. Description of a new technic and a preliminary report of its application. Circulation. 1964. 30:654–670.2. Lantis J, Jensen M, Benvenisty A, Mendes D, Gendics C, Todd G. Outcomes of combined superficial femoral endovascular revascularization and popliteal to distal bypass for patients with tissue loss. Ann Vasc Surg. 2008. 22:366–371.3. Diehm C, Schuster A, Allenberg JR, Darius H, Haberl R, Lange S, et al. High prevalence of peripheral arterial disease and comorbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis. 2004. 172:95–105.4. Newman AB, Shemanski L, Manolio TA, Cushman M, Mittelmark M, Polak JF, et al. The Cardiovascular Health Study Group. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. Arterioscler Thromb Vasc Biol. 1999. 19:538–545.5. Spinosa DJ, Leung DA, Matsumoto AH, Bissonette EA, Cage D, Harthun NL, et al. Percutaneous intentional extraluminal recanalization in patients with chronic critical limb ischemia. Radiology. 2004. 232:499–507.6. Fusaro M, Dalla Paola L, Biondi-Zoccai G. Pedal-plantar loop technique for a challenging below-the-knee chronic total occlusion: a novel approach to percutaneous revascularization in critical lower limb ischemia. J Invasive Cardiol. 2007. 19:E34–E37.7. Ingle H, Nasim A, Bolia A, Fishwick G, Naylor R, Bell PR, et al. Subintimal angioplasty of isolated infragenicular vessels in lower limb ischemia: long-term results. J Endovasc Ther. 2002. 9:411–416.8. Axisa B, Fishwick G, Bolia A, Thompson MM, London NJ, Bell PR, et al. Complications following peripheral angioplasty. Ann R Coll Surg Engl. 2002. 84:39–42.9. Lam RC, Shah S, Faries PL, McKinsey JF, Kent KC, Morrissey NJ. Incidence and clinical significance of distal embolization during percutaneous interventions involving the superficial femoral artery. J Vasc Surg. 2007. 46:1155–1159.10. Looby S, Keeling AN, McErlean A, Given MF, Geoghegan T, Lee MJ. Efficacy and safety of the angioseal vascular closure device post antegrade puncture. Cardiovasc Intervent Radiol. 2008. 31:558–562.11. Fantoni C, Medda M, Mollichelli N, Neagu A, Briganti S, Lo Monaco F, et al. Clip-based arterial haemostasis after antegrade common femoral artery puncture. Int J Cardiol. 2008. 29:427–429.12. Marcus AJ, Lotzof K, Howard A. Access to the superficial femoral artery in the presence of a "hostile groin": a prospective study. Cardiovasc Intervent Radiol. 2007. 30:351–354.13. Blais C. Antegrade puncture of the superficial femoral artery: a pilot project. Can Assoc Radiol J. 1993. 44:253–256. [French].14. Duda SH, Wiskirchen J, Erb M, Schott U, Khaligi K, Pereira PL, et al. Suture-mediated percutaneous closure of antegrade femoral arterial access sites in patients who have received full anticoagulation therapy. Radiology. 1999. 210:47–52.15. Nice C, Timmons G, Bartholemew P, Uberoi R. Retrograde vs. antegrade puncture for infra-inguinal angioplasty. Cardiovasc Intervent Radiol. 2003. 26:370–374.16. Biondi-Zoccai GG, Fusaro M, Tashani A, Mollichelli N, Medda M, De Giacobbi G, et al. Angioseal use after antegrade femoral arteriotomy in patients undergoing percutaneous revascularization for critical limb ischemia: a case series. Int J Cardiol. 2007. 118:398–399.17. Chiu AH, Vander Wal R, Tee K, Knight R, Coles SR, Nadkarni S. Comparison of arterial closure devices in antegrade and retrograde punctures. J Endovasc Ther. 2008. 15:315–321.18. Noory E, Rastan A, Sixt S, Schwarzwälder U, Leppännen O, Schwarz T, et al. Arterial puncture closure using a clip device after transpopliteal retrograde approach for recanalization of the superficial femoral artery. J Endovasc Ther. 2008. 15:310–314.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Tract Aortic Revascularization Technique in the Treatment of Aortoiliac Occlusive Disease
- Knotting and Kinking of the Guidewire during Central Venous Catheterization: A Case Report
- Tourniquet Occlusion Technique for Infrapopliteal Artery Revascularization
- Fatal Subacute Stent Thrombosis Induced by Guidewire Fracture with Retained Filaments in the Coronary Artery
- Usefulness of the double-guidewire technique for endoscopic procedures in the field of biliary and pancreatic diseases
