Percutaneous Placement of Self-expandable Metallic Biliary Stents in Malignant Extrahepatic Strictures: Indications of Transpapillary and Suprapapillary Methods
- Affiliations
-
- 1Department of Radiology, Yong-dong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. stent@medikorea.net
- KMID: 966475
- DOI: http://doi.org/10.3348/kjr.2000.1.2.65
Abstract
OBJECTIVE
To compare the efficacy of suprapapillary and transpapillary meth-ods of transhepatic biliary metallic stent placement in malignant biliary strictures and to specify the indications of each method applied. MATERIALS AND METHODS: Stents were placed in 59 patients. Strictures were cat-egorized as type A (within 3 cm of the ampulla, n = 27), type B (over 3 cm from ampulla, n = 7), type C (within 3 cm of the bending portion, n = 9), or type D (over 3 cm above the bending portion, n=16). The stenting method was suprapapillary in 34 cases and transpapillary in 25. The rates of initial and long-term patency and of early recurrence were compared. RESULTS: Initial patency rates for the suprapapillary and transpapillary methods were 1/7 (14.3%) and 20/20 (100%) respectively for type A (p < 0.0001), 4/5 (80.0%) and 2/2 for type B, 3/7 (42.9%) and 2/2 for type C, and 15/16 (93.8%) and 0/0 for type D. Early recurrence rates were 7/30 (23.3%) using the suprapap-illary method and 4/29 (13.8%) using the transpapillary method (p = 0.51). The long-term patency rate did not differ significantly according to either type (p =0.37) or method (p = 0.62). CONCLUSION: For good initial patency, the transpapillary method is recommended for strictures of the distal extrahepatic duct near the ampulla and just above the bending portion. Long-term patency is not influenced by the stenting method employed.
Keyword
MeSH Terms
Figure
-

Fig. 1 Anatomically, the extrahepatic duct is not straight for its entire course. Varying degrees of angulation between the proximal and distal axes of the extrahepatic duct can be noted.
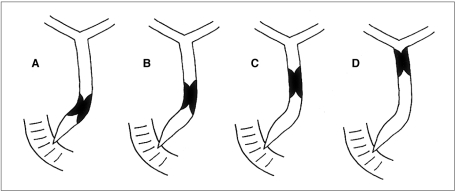
Fig. 2 Cholangiographic categorization of extrahepatic duct strictures according to location of distal margin of stricture within the bile duct and relationship with the angulation of the extrahepatic duct. (A) a stricture located within 3 cm of the ampulla (type A); (B) a stricture located more than 3 cm above the ampulla and at or below the bending portion (Type B); (C) a stricture located above the bending portion but within 3 cm of the bending portion (type C); (D) a stricture located over 3 cm from the bending portion (type D)
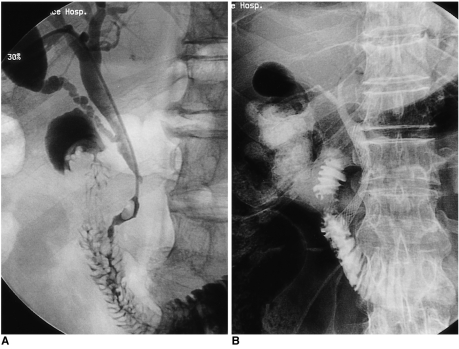
Fig. 3 A 65-year-old man with pancreatic head cancer.A. Because it was located within 3 cm of the ampulla of Vater, the stricture was categorized as type A.B. Using the transpapillary method of stent placement, the stricture was successfully palliated.
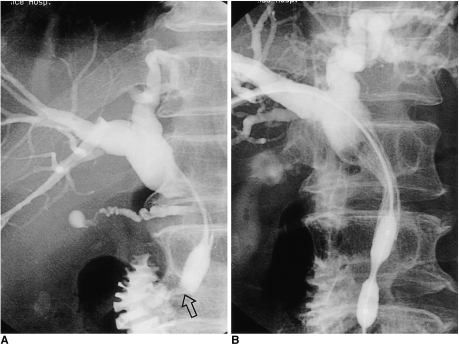
Fig. 4 A 52-year-old man with pancreatic head cancer.A. Because it was located within 3 cm of the ampulla of Vater, the stricture was categorized as type A. The passage of contrast medium injected via a catheter below the main stricture was good, and we therefore initially neglected a focal narrowing (open arrow) near the ampulla of Vater.B. The passage of contrast medium was poor after the suprapapillary method of stent placement was applied. The stricture was dilated using an angioplasty balloon catheter.

Fig. 5 A 62-year-old man presented with obstructed jaundice due to metastatic lymphadenopathy arising from advanced gastric cancer.A. Because it was located over 3 cm from the ampulla of Vater at the level of the bending portion of the extrahepatic duct, the stricture was categorized as type B.B. By means of the suprapapillary placement method, the stricture was successfully palliated.
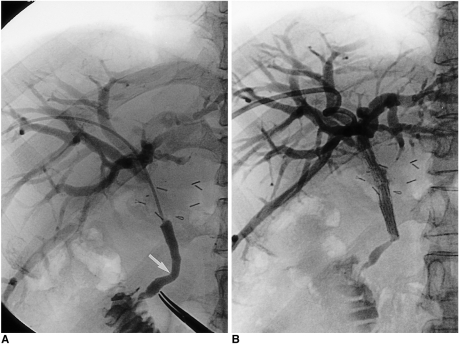
Fig. 6 A 56-year-old man with common hepatic duct cancer.A. Because it was located not more than 3 cm above the bending portion of the extrahepatic duct, the stricture was categorized as type C. Note the bending portion below the stricture (arrow).B. The stricture was palliated by means of the suprapapillary placement method. A cholangiogram obtained the following day demonstrated, however, that the angulation below the stricture was aggravated by the stretching effect of the stent. Note the presence of a significantly dilated intrahepatic duct, indicating poor passage of contrast medium through the extrahepatic duct.
Reference
-
1. Wilson MW. The application of metallic stents in malignant biliary obstruction. Tech in vasc Intervent Radiol. 1999; 2:39–52.
Article2. Gordon RL, Ring EJ, LaBerge JM, Doherty MM. Malignant biliary obstruction: treatment with expandable metallic stents-follow up of 50 consecutive patients. Radiology. 1992; 182:697–701. PMID: 1371362.3. Lee BH, Choe DH, Lee JH, Kim KH, Chin SY. Metallic stents in malignant biliary obstruction: prospective long-term clinical results. AJR. 1997; 168:741–745. PMID: 9057527.
Article4. Lameris JS, Stocker J, Nijs HG, et al. Malignant biliary obstruction: percutaneous use of self-expandable stents. Radiology. 1991; 179:703–707. PMID: 2027978.
Article5. Becker CD, Glattli A, Maibach R, Baer HU. Percutaneous palliation of malignant obstructive jaundice with the Wallstent endoprosthesis: follow-up and reintervention in patients with hilar and non-hilar obstruction. J Vasc Intervent Radiol. 1993; 4:597–604.
Article6. Lee MJ, Dawson SL, Mueller PR, et al. Percutaneous management of hilar biliary malignancies with metallic endoprostheses: results, technical problems, and causes of failure. RadioGraphics. 1993; 13:1249–1263. PMID: 8290722.
Article7. Lee BH, Do YS, Byun HS, Kim KH, Jin SY. Metallic stents for management of malignant biliary obstruction. J Korean Radiol Soc. 1992; 28:959–967.
Article8. Murphy BL, Mueller PR. Metallic biliary stents: technical points on optimizing results. Semin Intervent Radiol. 1996; 13:55–67.
Article9. Liu Q, Khay G, Cotton B. Feasibility of stent placement above the sphincter of Oddi ("Inside-Stent") for patients with malignant biliary obstruction. Endoscopy. 1998; 30:687–690. PMID: 9865557.
Article10. Stoker J, Lameris JS. Complications of percutaneously inserted biliary Wallstents. J Vasc Intervent Radiol. 1993; 4:767–772.
Article11. Dawson SL, Lee MJ, Mueller PR. Metal endoprostheses in malignant biliary obstruction. Semin Intervent Radiol. 1991; 8:242–251.
Article12. Roebuck DJ, Stanley P, Katz MD, Parry RL, Haight MA. Gastrointestinal hemorrhage due to duodenal erosion by a biliary Wallstent. Cardiovasc Intervent Radiol. 1998; 21:63–65. PMID: 9473549.
Article13. Van Steenbergen W, Van Aken L, Ponette E. Acute pancreatitis complicating the insertion of a self-expandable biliary metal stent. Endoscopy. 1992; 24:440–442. PMID: 1505495.
Article14. Yarze JC, Poulos AM, Fritz HP, Herlihy KJ. Treatment of metallic biliary stent-induced duodenal ulceration using endoscopic laser therapy. Dig Dis Sci. 1997; 42:6–9. PMID: 9009109.15. Ee H, Laurence BH. Haemorrhage due to erosion of a metal biliary stent through the duodenal wall. Endoscopy. 1992; 24:431–432. PMID: 1505493.
Article16. Bismuth H. Blumgast LH, editor. Postoperative strictures of the bile duct. The biliary tract. 1982. Edinburgh: Churchill Livingstone;p. 207–218.17. Lee BH, Do YS, Lee JH, Kim KH, Chin SY. New self-expandable spiral metallic stent: preliminary clinical evaluation in malignant biliary obstruction. J Vasc Intervent Radiol. 1995; 6:635–640.
Article18. Lindner HH. Clinical anatomy. 1989. Connecticut: Appleton & Lange;p. 418–422.19. Huibregtse K. The Wallstent for malignant biliary obstruction. Gastrointest Endosc Clin North Am. 1999; 9:491–501.
Article20. Lee BH, Kim KH, Chin SY. Mechanical characteristics of self-expandable metallic stents: in vitro study with three types of stresses. J Korean Radiol Soc. 1998; 39:497–502.21. Roh HG, Kang SG, Cho YK, et al. Physical property and MR imaging of self-expandable metallic stents. J Korean Radiol Soc. 1998; 39:503–509.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prophylactic endoscopic transpapillary gallbladder stenting to prevent acute cholecystitis induced after metallic stent placement for malignant biliary strictures: a retrospective study in Japan
- Current Status of Biliary Metal Stents
- Percutaneous placement of self-expandable metallic stents in patients with obstructive jaundice due to hepatocellular carcinoma
- Biliary Endoprosthese by the Use of Expandable Metallic Stents
- Complex percutaneous biliary procedures: Review and contributions of a high volume team
