Korean J Lab Med.
2008 Jun;28(3):201-206. 10.3343/kjlm.2008.28.3.201.
Clinical Utility of Serum Pepsinogen Levels as a Screening Test of Atrophic Gastritis
- Affiliations
-
- 1Department of Laboratory Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. ljh117@catholic.ac.kr
- 2Department of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 854867
- DOI: http://doi.org/10.3343/kjlm.2008.28.3.201
Abstract
- BACKGROUND
Atrophic gastritis is a well known risk factor for gastric adenocarcinoma. Its confirmatory diagnosis requires histology via endoscopy, which is an invasive method; therefore, periodic follow up evaluation as a screening method is difficult to perform. We evaluated the clinical utility of serum pepsinogens (PG) as a biomarker for screening of atrophic gastritis.
METHODS
The study population consisted of 130 selected dyspeptic patients (M:F=52:78; age, 16-105 yrs; mean age, 50.8 yrs) who had undergone a diagnostic endoscopy. The serum pepsinogen test was performed by a latex turbidimetric immunoassay method (HBI, Korea) using Toshiba-200FR automatic analyzer. The PGI, II level and PGI:PGII ratio of non-atrophic gastritis group were compared with those of atrophic gastritis group, and a correlation with Helicobacter pylori infection was examined. Cut-off points for screening of atrophic gastritis were determined.
RESULTS
The mean serum concentration of PGI showed a decline from normal (60.7 ng/mL), nonatrophic gastritis (54.2 ng/mL), and atrophic gastritis (51.8 ng/mL) to gastric adenocarcinoma (32.6 ng/mL). The mean ratio of PGI:PGII was lower in atrophic gastritis (3.2) compared to non-atrophic gastritis (4.7) (P=0.021). In patients with H. pylori infection, the mean serum PGII level was higher and the PGI:PGII ratio was lower than those in patients without H. pylori infection, and the differences were statistically significant. For screening of atrophic gastritis, the best cut-off point of PGI:PGII ratio was 4, with a sensitivity of 82.6% and specificity of 91.7%.
CONCLUSIONS
The serum pepsinogen test is a useful biomarker for screening of atrophic gastritis, a well-known precancerous lesion of gastric adenocarcinoma. Measuring both pepsinogen I and II concentrations simultaneously to obtain pepsinogen I/II ratio provides a clinically useful information for the detection of atrophic gastritis.
MeSH Terms
Figure
-
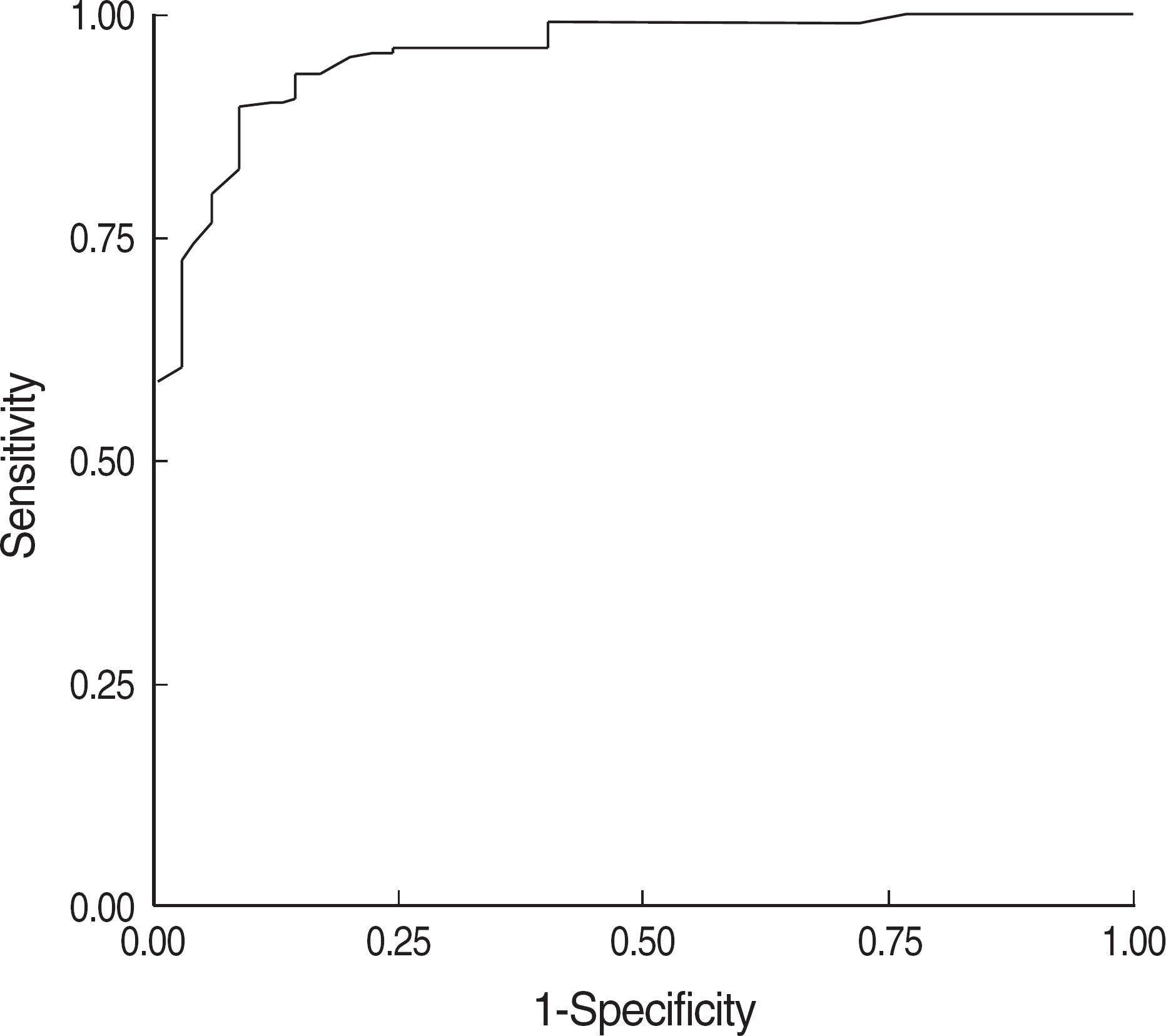
Fig. 1. Receiver operating curve (ROC) for pepsinogen I/II ratio for screening of atrophic gastritis (cut-off value: pepsinogen I/II ratio <4, sensitivity: 82.6%, specificity: 91.7%).
Reference
-
1.Shin HR., Jung KW., Won YJ., Park JG. 2002 annual report of Korea central cancer resistry: based on registered data from 139 hospitals. Cancer Res Treat. 2004. 36:103–14.2.Sipponen P., Kekki M., Haapakoski J., Ihamaki T., Siurala M. Gastric cancer risk in chronic atrophic gastritis: statistical calculations of cross-sectional data. Int J Cancer. 1985. 35:173–7.3.Di Gregorio C., Morandi P., Fante R., De Gaetani C. Gastric dysplasia. A follow-up study. Am J Gastroenterol. 1993. 88:1714–9.4.Samloff IM. Cellular localization of group I pepsinogens in human gastric mucosa by immunofluorescence. Gastroenterology. 1971. 61:185–8.
Article5.Samloff IM., Liebman WM. Cellular localization of the group II pepsinogens in human stomach and duodenum by immunofluorescence. Gastroenterology. 1973. 65:36–42.
Article6.Korstanje A., den Hartog G., Biemond I., Lamers CB. The serological gastric biopsy: a non-endoscopical diagnostic approach in management of the dyspeptic patient: significance for primary care based on a survey of the literature. Scand J Gastroenterol Suppl. 2002. 236(S):S22–6.
Article7.Mukoubayashi C., Yanaoka K., Ohata H., Arii K., Tamai H., Oka M, et al. Serum pepsinogen and gastric cancer screening. Intern Med. 2007. 46:261–6.
Article8.Sipponen P., Harkonen M., Alanko A., Suovaniemi O. Diagnosis of atrophic gastritis from a serum sample. Clin Lab. 2002. 28:505–15.9.Lorente S., Doiz O., Trinidad Serrano M., Castillo J., Lanas A. Helicobacter pylori stimulates pepsinogen secretion from isolated human peptic cells. Gut. 2002. 50:13–8.
Article10.Fukuda H., Saito D., Hayashi S., Hisai H., Ono H., Yoshida S, et al. Helicobacter pylori infection, serum pepsinogen level and gastric cancer: a case-control study in Japan. Jpn J Caner Res. 1995. 86:64–71.11.Miki K., Urita Y. Using serum pepsinogens wisely in a clinical practice. J Dig Dis. 2007. 8:8–14.
Article12.Paik CN., Chung IS., Nam KW., Kwon JH., Chang JH., Suh JP, et al. Relationship between pepsinogen I/II ratio and age or upper gastrointestinal diseases in Helicobacter pylori-positive and negative subjects. Korean J Gastroenterol. 2007. 50:84–91. (백창렬, 정인식, 남관우, 권정현, 장재혁, 서정필 등. Helicobacter pylori 양성, 음성 환자에서각종상부위장관질환과나이에따른펩시노겐 I/II 비. 대한소화기학회지 2007;50: 84-91.).13.Broutet N., Plebani M., Sakarovitch C., Sipponen P., Megraud F. Eurohepygast Study Group. Pepsinogen A, pepsinogen C, and gastrin as markers of atrophic chronic gastritis in European dyspeptics. Br J Cancer. 2003. 88:1239–47.
Article14.Miki K., Ichinose M., Shimizu A., Huang SC., Oka H., Furihata G, et al. Serum pepsinogens as a screening test of extensive chronic gastritis. Gastroenterol Jpn. 1987. 22:133–41.
Article15.Kitahara F., Kobayashi K., Sato T., Kojima Y., Araki T., Fujino AM. Accuracy of screening for gastric cancer. J Gastroenterol. 1995. 30:452–60.16.Aoki K., Misumi J., Kimura T., Zhao W., Xie T. Evaluation of cutoff levels for screening of gastric cancer using serum pepsinogens and distributions of levels of serum pepsinogen I, II and of PG I/PG II ratios in a gastric cancer case-control study. J Epidemiol. 1997. 7:143–51.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changing Trends of Serum Pepsinogen I/II Ratio in Asymptomatic Subjects
- Serum Pepsinogen l, ll Levels and Upper Gastrointestinal Diseases in Children with H. pylori Infection
- Comparison of Intestinal Metaplasia and Serum Pepsinogen Levels between Helicobacter pylori-Infected Duodenal Ulcer and Chronic Gastritis
- The Role of Serum Pepsinogen and Gastrin Test for the Detection of Gastric Cancer in Korea
- Endoscopic gastritis, serum pepsinogen assay, and Helicobacter pylori infection
