Part-Time Occlusion Therapy for Anisometropic Amblyopia Detected in Children Eight Years of Age and Older
- Affiliations
-
- 1Department of Ophthalmology, Hallym University College of Medicine, Chunchon Sacred Heart Hospital, Chunchon, Korea.
- 2Department of Ophthalmology, Hallym University College of Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea. ljy690725@hanmail.net
- KMID: 754575
- DOI: http://doi.org/10.3341/kjo.2006.20.3.171
Abstract
- PURPOSE: To determine the outcome of part-time occlusion therapy in children with anisometropic amblyopia detected after they were 8 years of age. METHODS: We analyzed 29 eyes with anisometropic amblyopia in children 8 years of age and older. The mean age was 8.79+/-0.98 (range 8~12) years old. The subjects whose best-corrected visual acuity (BCVA) did not improve by two lines or better within 2 weeks of wearing glasses full-time were prescribed occlusion therapy for 6 hours a day outside of school hours, along with the instruction to wear glasses full-time. Subjects who complied with occlusion for more than 3 hours a day were considered to comply well. RESULTS: The major component of the anisometropia was hyperopia in 51.7% of the subjects, and hyperopia plus astigmatism was found in 24.1%. The mean pretreatment BCVA score was 0.51+/-0.23 (LogMAR). Compliance was 89.66%. The mean posttreatment BCVA was 0.03+/-0.01 (LogMAR), and the success rate, based on a posttreatment BCVA of 0.1 (LogMAR) and better, was 96.43%. It took an average of 4.79+/-3.35 months to reach the desired posttreatment BCVA. The mean posttreatment stereopsis was 79.78+/-37.61 seconds of arc. The recurrence rate was 8%. The visual improvement was related to the degree of compliance (p=0.000). The time taken to reach the posttreatment BCVA was shorter in subjects with a better pretreatment BCVA (p=0.019), but it did not relate to the compliance (p=0.366). CONCLUSIONS: The most common component of anisometropia detected after 8 years of age was hyperopia. The part-time occlusion therapy, which had been carried out after school hours, was successful in most cases.
MeSH Terms
Figure
-
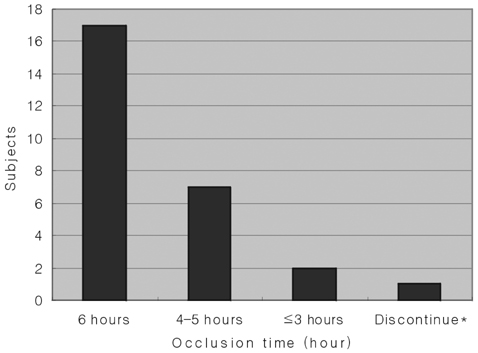
Fig. 1 Distribution of the daily occlusion hours. When subjects who had covered their strong eyes for more than 3 hours a day were considered to comply well, the compliance of part-time occlusion therapy was 88.9%. *: One subject disontinued the occlusion therapy before his corrected visual acuity reached the plateau.
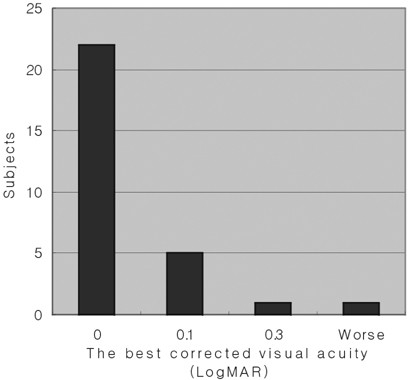
Fig. 2 Distribution of posttreatment best-corrected visual acuities. The mean was LogMAR 0.03±0.01. The success rate was 93.1% based on the cases where the final best-corrected visual acuity was 0.8 (LogMAR=0.1) or higher.
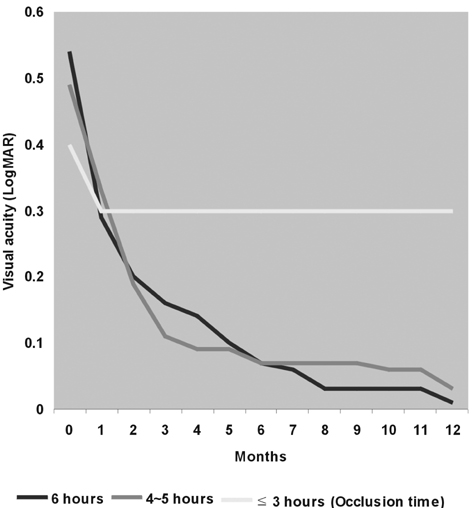
Fig. 3 The graph of monthly visual acuity changes according to the occlusion time.
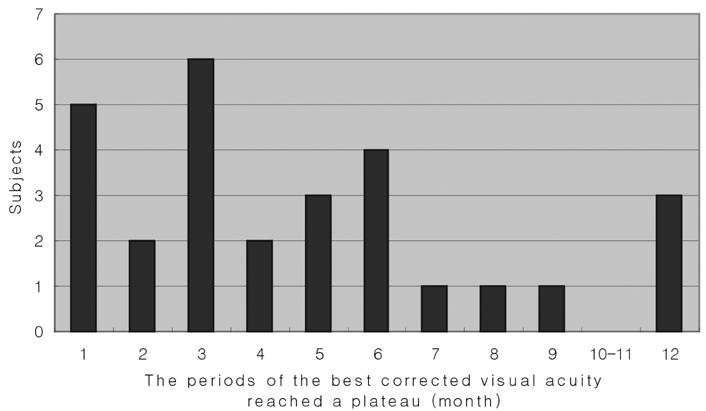
Fig. 4 The period of occlusion therapy determined by the time at which the pretreatment best-corrected visual acuity reached a plateau of its best level. In most cases it took less than 6 months, and the mean period of occlusion therapy was 4.79±3.35 months.
Reference
-
1. Duke-Elder S, Wybar K. Ocular motility and strabismus. 1973. 1st ed. St Louis: CV Mosby, Kimpton;294.2. Leguire LE, Komaromy KL, Nairus TM, Rogers GL. Long-term follow-up of L-dopa treatment in children with amblyopia. J Pediatr Ophthalmol Strabismus. 2002. 39:326–330.3. Pandey PK, Chaudhuri Z, Kumar M, et al. Effect of levodopa and carbidopa in human amblyopia. J Pediatr Ophthalmol Strabismus. 2002. 39:81–89.4. Von Noorden GK. Classification of amblyopia. Am J Ophthalmol. 1967. 63:238–244.5. Jin YH. Strabismology. 1999. 2nd ed. Ulsan: Ulsan University Press;205–229.6. Kim YT, Chang HR. Follow-up Results of the Monocular Amblyopia. J Korean Ophthalmol Soc. 1998. 39:305–311.7. Park MH, Rah SH, Kim SH. The analysis of improvement of visual acuity by occlusion therapy in amblyopic children above 6 years of age. J Korean Ophthalmol Soc. 1994. 35:190–195.8. Yeom HY, Han SH, Lee JB. Effects of solitary part-time occlusion for the treatment of monocular amblyopia patients. J Korean Ophthalmol Soc. 2004. 45:1134–1140.9. Scott WE, Stratton VB, Fabre J. Full-time occlusion therapy for amblyopia. Am Orthopt J. 1980. 30:125–130.10. Moon CS, Jin YH. Timing of amblyopia therapy in pure anisometropic amblyopia. J Korean Ophthalmol Soc. 1998. 39:185–192.11. Repka MX, Cotter SA, Beck RW, et al. A Randomized trial of atropine regimens for treatment of moderate amblyopia in children. Ophthalmology. 2004. 111:2076–2085.12. Sloan LL. Measurement of visual acuity. AMA Arch Ophthalmol. 1951. 45:704–725.13. Von Noorden GK, Campos EC. Binocular vision and Ocular motility. 2002. 6th ed. St. Louis: Mosby;246–287.14. Hiscox F, Strong N, Thompson JR, et al. Occlusion for amblyopia a comprehensive survey of outcome. Eye. 1992. 6:300–304.15. The Pediatric Eye Disease Investigator Group. A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthalmol. 2003. 121:603–611.16. Epelbaum M, Milleret C, Buisseret P, Dufier JL. The sensitive period for strabismic amblyopia in humans. Ophthalmology. 1993. 100:323–327.17. Flynn JT, Schiffman J, Feuer W, Corona A. The therapy of amblyopia: an analysis of the results of amblyopia therapy utilizing the pooled data of publishied studies. Trans Am Ophthalmol Soc. 1998. 96:431–450.18. Rutstein RP, Fuhr PS. Efficacy and stability of amblyopia therapy. Optom Vis Sci. 1992. 69:747–754.19. Oliver M, Neumann R, Chaimovitch Y, et al. Compliance and results of treatment for amblyopia in children more than 8 years old. Am J Ophthalmol. 1986. 102:340–345.20. Mohan K, Saroha V, Sharma A. Successful occlusion therapy for amblyopia in 11- to 15-year-old children. J Pediatr Ophthalmol Strabismus. 2004. 41:89–95.21. Park KH, Hwang JM, Ahn JK. Efficacy of amblyopia therapy initiated after 9 years of age. Eye. 2004. 18:571–574.22. Searle A, Norman P, Harrad R, Vedhara K. Psychosocial and clinical determinants of compliance with occlusion therapy for amblyopic children. Eye. 2002. 16:150–155.23. Beardsell R, Clarke S, Hill M. Outcomes of occlusion treatment for amblyopia. J Pediatr Ophthalmol Strabismus. 1999. 36:19–24.24. Roh GH, Cho YA. Compliance of patching therapy for amblyopia. J Korean Ophthalmol Soc. 1993. 34:103–109.25. The Pediatric Eye Disease Investigator Group. Risk of amblyopia recurrence after cessation of treatment. J AAPOS. 2004. 8:420–428.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effects of Occlusion Therapy in Patients With Anisometropic Amblyopia Aged 8 Years and Older
- The clinical outcomes of Occlusion for Monocular Amblyopia in Children More than 8 years
- The Effect of L-dopa in Amblyopic Children for Whom Occlusion Therapy Failed
- Efficacy of Occlusion Therapy in Amblyopia Patients Older than 9 Years of Age
- Efficacy of Occlusion Therapy in Amblyopia: Type, Depth and Timing of Amblyopia
