The Spectrum of Benign Esophageal Lesions: Imaging Findings
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kslee@smc.samsung.co.kr
- 2Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 754063
- DOI: http://doi.org/10.3348/kjr.2002.3.3.199
Abstract
- Benign esophageal lesions occur in various diseases. Barium studies are useful for the evaluation of mucosal surface lesions but provide little information about the extramucosal extent of disease. Computed tomography and magnetic resonance imaging, on the other hand, permit the assessment of wall thickness, mediastinal involvement, adjacent lymphadenopathy, and distant spread. In diseases such as fibrovascular polyps, duplication cysts, scleroderma, trauma, caustic esophagitis, hiatal hernia, esophageal diverticulum, achalasia, and paraesophageal varices, the findings of imaging studies are specific, obviating the need for further invasive diagnostic work-up. The advent of helical computed tomography and its volume data set allows the acquisition of multiplanar images, and magnetic resonance imaging is useful both for this and for tissue characterization. Thus, multiplanar cross-sectional imaging further extends the role of imaging modalities to the evaluation of benign esophageal lesions. Through an awareness of the multiplanar cross-sectional appearances of various benign esophageal lesions, the radiologist can play an important role in the detection, diagnosis, further diagnostic planning, and treatment of the diseases in which they occur.
Keyword
MeSH Terms
Figure
-

Fig. 1 Esophageal leiomyoma in a 35-year-old woman. A. Chest radiograph shows a right retrocardiac soft-tissue mass (arrows), with obliteration of the azygoesophageal recess interface. B. Enhanced (10-mm collimation) CT scan obtained at the ventricular level depicts a 60-mm-sized, slightly inhomogeneous, iso-attenuated, pear-shaped mass (arrows) in the right azygoesophageal recess. C. T2-weighted MR image obtained at a similar level to B shows that compared to chest wall muscle, the mass is isointense (arrows).

Fig. 2 Giant fibrovascular polyp in a 52-year-old man. A. Esophagogram shows that the contrast-filled dilated esophageal lumen contains a large mass consisting of filling defects (arrows). The pedicle of the mass (curved arrows) is visible. B. Enhanced (10-mm collimation) conventional CT scan obtained at the level of the great vessels shows a round polypoid soft-tissue lesion (arrow) arising from the posterolateral wall of the thickened esophagus. The identity of the portion, thought preoperatively to be pedicle, was confirmed at surgery. C. CT scan obtained at the level of the distal main bronchi depicts a heterogeneous soft-tissue mass, posterior to the air-filled esophageal lumen (arrowhead). Fatty (arrows) and soft-tissue attenuation (curved arrows) is observed. D. Coronal T1-weighted MR image reveals an elongated lesion involving the entire esophagus. Compared to chest wall muscle, it shows central high (arrows) and peripheral iso-signal intensity (curved arrows). E. Axial T2-weighed image shows signal change in lesions compared to T1-weighted image (D); signal intensity is centrally low (arrows) and peripherally high (arrow heads). F. This fragment of excised mass consists mainly of fat (arrows), and is covered with normal esophageal mucosa (arrowheads). G. Photomicrograph (H & E staining, ×40) depicts intact stratified squamous epithelium (open arrows), fibrous tissue (asterisk), and numerous thin blood vessels (arrows).

Fig. 3 A 68-year-old man with tubular esophageal duplication. A. Mediastinal window of initial enhanced (10-mm collimation) CT scan obtained at the level of the aortopulmonary window shows two esophageal lumina : an air-filled smaller inner lumen (open arrow) is surrounded by a hematoma-filled larger outer lumen (closed arrow). A thin enhancing esophageal rim suggests the presence of mucosal lining. Also note the small lymph node in the left paratracheal area (arrowhead). B. Follow-up thin-section (1.5-mm collimation) CT scan obtained at a similar level to (A) shows that the outer lumen, previously filled with hematoma, is filled with air (curved arrow). A septum (arrow) still separates the lumina. C. Endoscopic examination reveals multiple and irregular communicating mucosal defects (arrows). D. Pathologic specimen with a longitudinally sliced wall and septum has two lumina (asterisks) separated along their entire course by a shaggy septum with multiple defects (arrows) (reprinted, with permission, from reference 18).
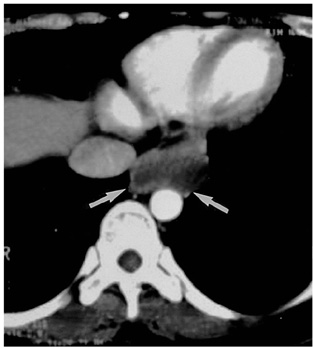
Fig. 4 A 50-year-old woman with cystic esophageal duplication. On this (7-mm collimation) CT scan obtained at the level of the liver dome, a homogeneous mass of low attenuation and with a smooth border (arrows) appears to the left of the inferior vena cava and anterior to the aorta.

Fig. 5 Esophageal schwannoma in a 70-year-old woman. A. Esophagogram depicts a large, smoothly elevated filling defect, and displacement of the distal esophagus. B. Enhanced (7-mm collimation) CT scan obtained at the level of the inferior pulmonary vein shows that a homogeneous, soft-tissue lesion (arrows), of low attenuation and measuring 60 × 50 mm in diameter, occupies the left posterior mediastinum.
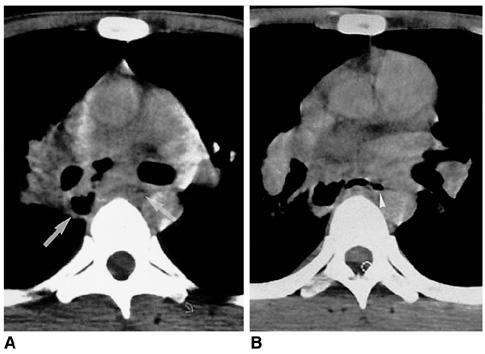
Fig. 6 Mediastinal tuberculous lymphadenitis with esophagomediastinal fistula in a 27-year-old man with AIDS. A, B. CT scans obtained at the levels of the left main bronchi (A) and the right superior segmental bronchus (B), respectively, reveal that within enlarged lymph nodes in the right subcarinal area, there are irregularly-shaped gas collections ( arrows) that communicate with esophageal gas (arrowhead in B).
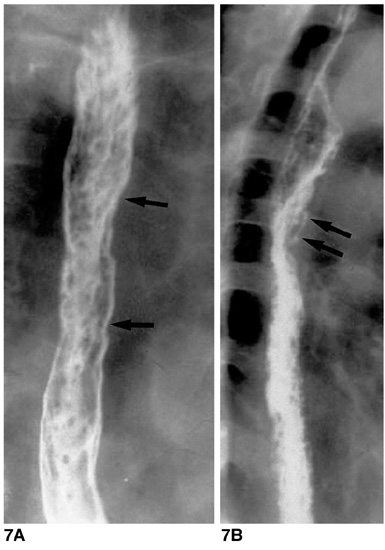
Fig. 7 Candida esophagitis in a 76-year-old man with diabetes mellitus. A. Double contrast esophagogram of the proximal esophagus has a cobblestone appearance (arrows) due to the coalescence of round, ovoid, and polygonal plaques. B. Esophagogram of the mid and distal esophagus has a shaggy appearance, and grossly irregular contour, due to the presence of multiple plaques and ulcers. Pseudomembrane (arrows) is seen as double tracts which parallel the esophagus.
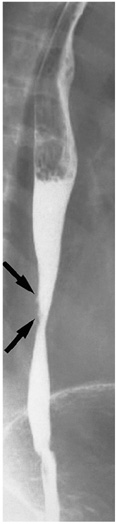
Fig. 8 Reflux esophagitis in a 42-year-old woman. Double-contrast esophagogram reveals smoothly tapered luminal narrowing of the distal esophagus, and the presence of a shallow linear ulcer (arrows).
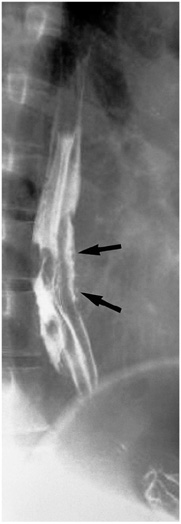
Fig. 9 Behcet's disease in a 44-year-old man. Double-contrast esophagogram demonstrates irregular shallow ulceration within irregularly thickened folds (arrows) of the distal esophagus.

Fig. 10 Esophageal involvement in a 59-year-old man with scleroderma. Lung window of thin-section (1-mm collimation) CT scan obtained at the level of the liver dome shows a dilated esophagus (arrows), a moderate amount of pericardial effusion (open arrows), and left pleural effusion (curved arrows). Also note the occurrence of pulmonary change consisting of irregular linear opacities, ground-glass opacities, and honeycombing.

Fig. 11 Spontaneous esophageal rupture in a 58-year-old man after heavy alcohol consumption. A. Esophagogram shows no evidence of contrast medium leakage, though mediastinal widening (arrows) is apparent. A nasogastric tube (arrowheads) was inserted. B. Mediastinal window of enhanced (7-mm collimation) CT scan obtained at the level of the aortic arch demonstrates widening of the right superior mediastinum (arrows), and extraluminal air. Also note that parenchymal consolidation (open arrows), probably due to passive atelectasis associated with mediastinal widening, has occurred in the right upper lobe.

Fig. 12 Esophagotracheal fistula in a 42-year-old woman with blunt trauma. A. Mediastinal window of unenhanced (7-mm collimation) CT scan obtained at the level of the distal trachea shows a fistulous tract (arrows) between the trachea and esophagus. The superior mediastinum is widened, and there is air and soft tissue attenuation (open arrows). Also note the presence of extensive subcutaneous emphysema in the anterior chest wall. B. Three-dimensional CT image using the shaded-surface display technique indicates that at the distal trachea, a fistulous tract (arrows) is present.
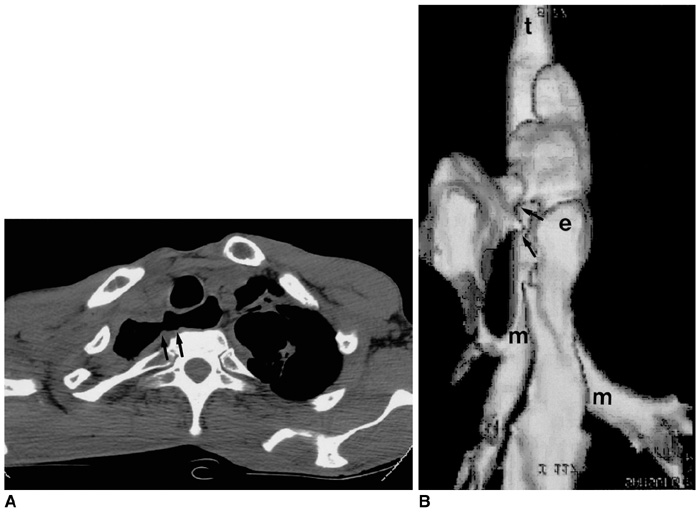
Fig. 13 Esophagopleural fistula in a 35-year-old man with chronic destructive pulmonary tuberculosis. A. Mediastinal window of unenhanced (7-mm collimation) CT scan obtained at the level of the thoracic inlet depicts a fistulous tract (arrows) between the proximal esophagus and right pleural space. B. Posteroanterior view of three-dimensional CT image using the shaded-surface display technique reveals the presence of fistulous tracts between the esophagus and right pleural space (arrows)(t = trachea, e = esophagus, m = main bronchus).
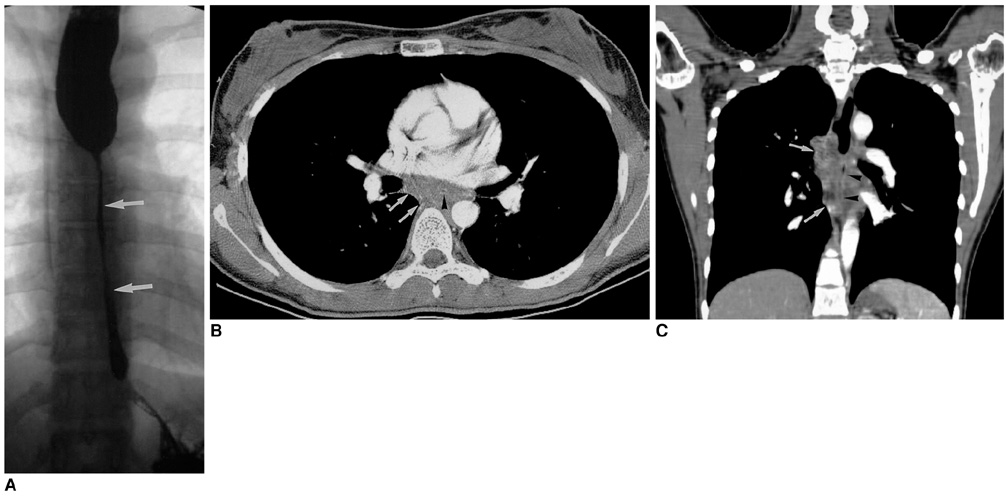
Fig. 14 Lye stricture in a 25-year-old man who ingested of liquid lye five years earlier. A. Esophagogram shows diffuse cord-like luminal narrowing (arrows) of the mid-to-distal esophagus. B. Mediastinal window of enhanced (2.5-mm collimation) CT scan obtained at the level of the distal bronchus intermedius reveals obliteration of the esophageal lumen (arrowhead) and periesophageal soft-tissue attenuation due to inflammatory and fibrotic change (arrows). C. Coronal reformatted (3-mm collimation) CT image shows slit-like luminal narrowing (arrowheads) of the subcarinal esophagus, with periluminal soft-tissue attenuation (arrows).
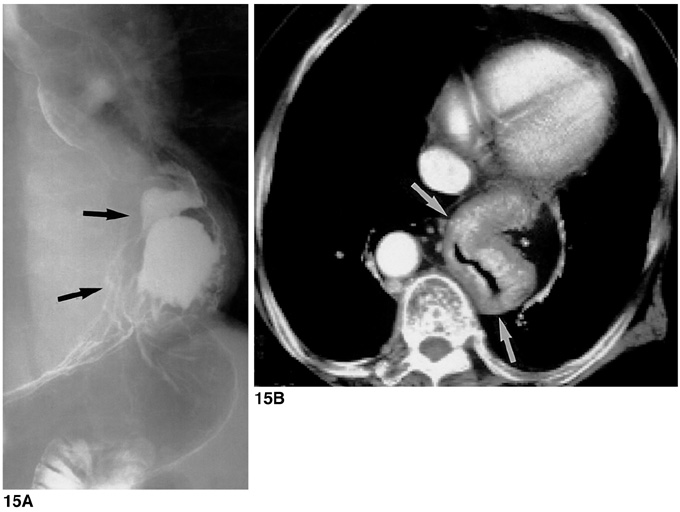
Fig. 15 Sliding hiatal hernia in a 30-year-old man. A. Esophagogram shows that a portion of stomach (arrows) lies above the diaphragm. B. Mediastinal window of enhanced (7-mm collimation) CT scan obtained at the level of the suprahepatic inferior vena cava shows that the thorax contains a portion of stomach (arrows). The aorta is displaced to the right.
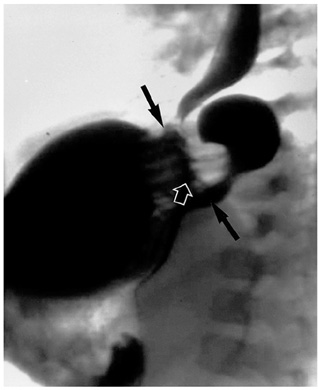
Fig. 16 Paraesophageal hernia in a 2-year-old boy. Esophagogram depicts elevated gastric fundus extending through the widened esophageal hiatus to the thoracic cavity (arrows). Note that the intra-abdominal position of the gastroesophageal junction (open arrow) is normal.
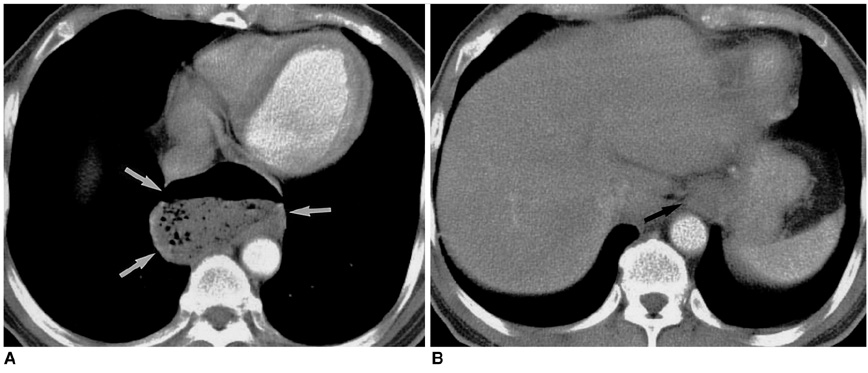
Fig. 17 Epiphrenic esophageal diverticulum in a 63-year-old man. A. Mediastinal window of enhanced (7-mm collimation) CT scan obtained at the level of the suprahepatic inferior vena cava shows that outpouching (arrows) from the esophagus contains an air-fluid level. B. CT scan obtained at the level of the liver dome shows that the position of the esophagogastric junction (arrow) is normal.
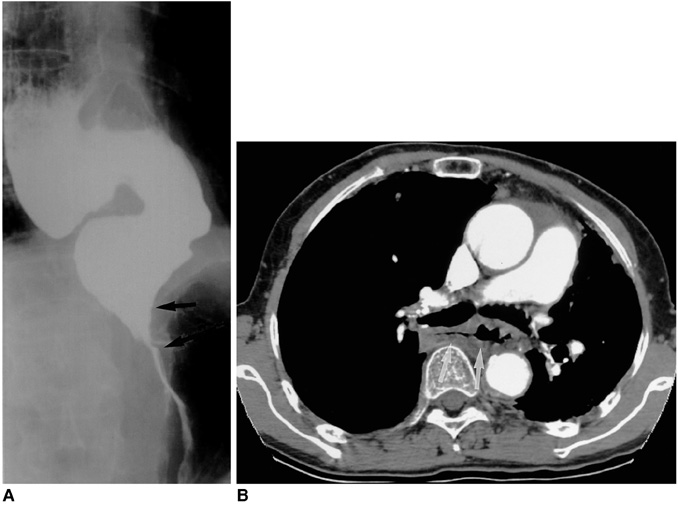
Fig. 18 Achalasia in a 50-year-old woman. A. Esophagogram demonstrates smoothly tapered, beak-like narrowing at the esophagogastric junction (arrows) and a diffuse dilated esophagus. B. Mediastinal window of enhanced (5-mm collimation) CT scan obtained at the level of the main bronchi shows a dilated esophagus (arrows), with mild diffuse wall thickening.
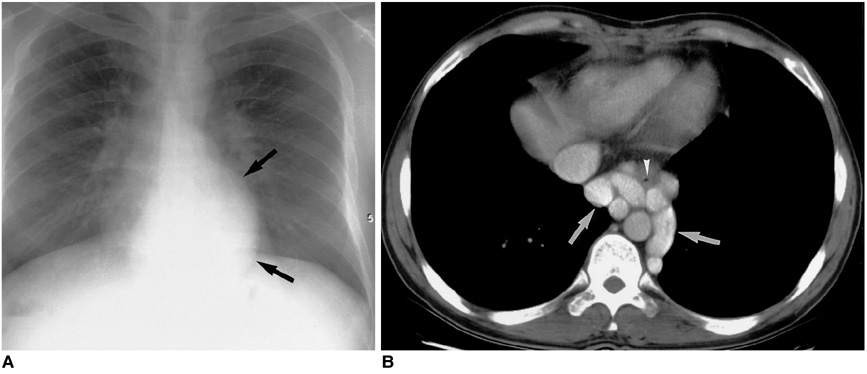
Fig. 19 Paraesophageal varices in a 45-year-old man with liver cirrhosis. A. Chest radiograph depicts a retrocardiac soft-tissue mass (arrows). B. Mediastinal window of enhanced (5-mm collimation) CT scan obtained at the level of the suprahepatic inferior vena cava shows enhancing tubular structures (arrows) surrounding the esophageal lumen (arrowhead).
Reference
-
1. Halber MD, Daffner RH, Thompson WM. CT of the esophagus: normal appearance. AJR. 1979. 133:1047–1050.2. Berkovich GY, Levine MS, Miller WT. CT findings in patients with esophagitis. AJR. 2000. 175:1431–1434.3. Seremetis MG, Lyons WS, DeGuzman VC, et al. Leiomyomata of the esophagus: an analysis of 838 cases. Cancer. 1976. 38:2166–2177.4. Cochat P, Guibaud P, Garcia Torres R, Roussel B, Guarner V, Larbre F. Diffuse leiomyomatosis in Alport syndrome. J Pediatr. 1988. 113:339–343.5. Yang PS, Lee KS, Lee SJ, et al. Esophageal leiomyoma: radiologic findings in 12 patients. Korean J Radiol. 2001. 2:132–137.6. Levine MS, Buck JL, Pantongrag-Brown L, Buetow PC, Hallman JR, Sobin LH. Fibrovascular polyps of the esophagus: clinical, radiographic, and pathologic findings in 16 patients. AJR. 1996. 166:781–787.7. Cochet B, Hohl P, Sans M, et al. Asphyxia caused by laryngeal impaction of an esophageal polyp. Arch Otoloaryngol. 1980. 106:176–178.8. Stoane JM, Torrisi JM, Haller JO, David M. Fibrovascular polyps of the esophagus: MRI findings. J Comput Assist Tomogr. 1995. 19:157–159.9. Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. RadioGraphics. 1993. 13:1063–1080.10. Kim YS, Park CK, Choi YW, Jeon SC, Seo HS, Hahm CK. Esophageal tubular duplication complicated by intraluminal hematoma: a case report. J Korean Med Sci. 2000. 15:463–466.11. Kuhlman JE, Fishman EK, Wang KP, Siegelman SS. Esophageal duplication cyst: CT and transesophageal needle aspiration. AJR. 1985. 145:531–532.12. Saito R, Kitamura M, Suzuki H, Ogawa J, Sageshima M. Esophageal schwannoma. Ann Thorac Surg. 2000. 69:1947–1949.13. Ueyama T, Guo KJ, Hashimoto H, Daimaru Y, Enjoji M. Benign schwannoma of the gastrointestinal tract: a clinicopathologic and immunohistochemical study. Hum Pathol. 1988. 19:257–264.14. Im J-G, Kim JH, Han MC, Kim CW. Computed tomography of esophagomediastinal fistula in tuberculous mediastinal lymphadenitis. J Comput Assist Tomogr. 1990. 14:89–92.15. Levine MS, Macones AJ Jr, Laufer I. Candida esophagitis: accuracy of radiographic diagnosis. Radiology. 1985. 154:581–587.16. Vahey TN, Maglinte DD, Chernish SM. State-of-the-art barium examination in opportunistic esophagitis. Dig Dis Sci. 1986. 31:1192–1195.17. Graziani L, De Nigris E, Pesaresi A, Baldelli S, Dini L, Montesi A. Reflux esophagitis: radiologic-endoscopic correlation in 39 symptomatic cases. Gastrointest Radiol. 1983. 8:1–6.18. Laufer I. Radiology of esophagitis. Radiol Clin North Am. 1982. 20:687–699.19. Levine MS. Barrett's esophagus: a radiologic diagnosis? AJR. 1988. 151:433–438.20. Reid BJ. Barrett's esophagus and esophageal adenocarcinoma. Gastroenterol Clin North Am. 1991. 20:817–834.21. Mori S, Yoshihira A, Kawamura H, Takeuchi A, Hashimoto T, Inaba G. Esophageal involvement in Behcet's disease. Am J Gastroenterol. 1983. 78:548–553.22. Bhalla M, Silver RM, Shepard JO, McLoud TC. Chest CT in patients with scleroderma. AJR. 1993. 161:269–272.23. Pasricha PJ, Fleischer DE, Kalloo AN. Endoscopic perforations of the upper digestive tract: a review of their pathogenesis, prevention, and management. Gastroenterology. 1994. 106:787–802.24. Backer CL, LoCicero J, Hartz RS, Donaldson JS, Shields T. Computed tomography in patients with esophageal perforation. Chest. 1990. 98:1078–1080.25. Berkman YM, Auh YH. CT diagnosis of acquired tracheoesophageal fistula in adults. J Comput Assist Tomogr. 1985. 9:302–304.26. Wechsler RJ. CT of esophageal-pleural fistulae. AJR. 1986. 147:907–909.27. Appelqvist P, Salmo M. Lye corrosion carcinoma of the esophagus: a review of 63 cases. Cancer. 1980. 45:2655–2685.28. Lindell MM Jr, Bernardino ME. Diagnosis of hiatus hernia by computed tomography. J Comput Assist Tomogr. 1981. 5:16–19.29. Kim KW, Berkmen YM, Auh YH, Kazam E. Diagnosis of epiphrenic esophageal diverticulum by computed tomography. J Comput Assist Tomogr. 1988. 12:25–28.30. Rabushka LS, Fishman EK, Kuhlman JE. CT evaluation of achalasia. J Comput Assist Tomogr. 1991. 15:434–439.31. Tishler JM, Shin MS, Stanley RJ, Koehler RE. CT of the thorax in patients with achalasia. Dig Dis Sci. 1983. 28:692–697.32. Hirose J, Takashima T, Suzuki M, Matsui O. "Downhill" esophageal varices demonstrated by dynamic computed tomography. J Comput Assist Tomogr. 1984. 8:1007–1009.33. Balthazar EJ, Naidich DP, Megibow AJ, Lefleur RS. CT evaluation of esophageal varices. AJR. 1987. 148:131–135.34. Lee SJ, Lee KS, Kim SA, Kim TS, Hwang JH, Lim JH. Computed radiography of the chest in patients with paraesophageal varices: diagnostic accuracy and characteristic findings. AJR. 1998. 170:1527–1531.
