Ruptured Corpus Luteal Cyst: CT Findings
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine Institute of Radiation Medicine. kimsh@radcom.snu.ac.kr
- KMID: 754041
- DOI: http://doi.org/10.3348/kjr.2003.4.1.42
Abstract
OBJECTIVE
To evaluate the CT findings of ruptured corpus luteal cysts. MATERIALS AND METHODS: Six patients with a surgically proven ruptured corpus luteal cyst were included in this series. The prospective CT findings were retrospectively analyzed in terms of the size and shape of the cyst, the thickness and enhancement pattern of its wall, the attenuation of its contents, and peritoneal fluid. RESULTS: The mean diameter of the cysts was 2.8 (range, 1.5-4.8) cm; three were round and three were oval. The mean thickness of the cyst wall was 4.7 (range, 1-10) mm; in all six cases it showed strong enhancement, and in three was discontinuous. In five of six cases, the cystic contents showed high attenuation. Peritoneal fluid was present in all cases, and its attenuation was higher, especially around the uterus and adnexa, than that of urine present in the bladder. CONCLUSION: In a woman in whom CT reveals the presence of an ovarian cyst with an enhancing rim and highly attenuated contents, as well as highly attenuated peritoneal fluid, a ruptured corpus luteal cyst should be suspected. Other possible evidence of this is focal interruption of the cyst wall and the presence of peritoneal fluid around the adnexa.
Keyword
Figure
-
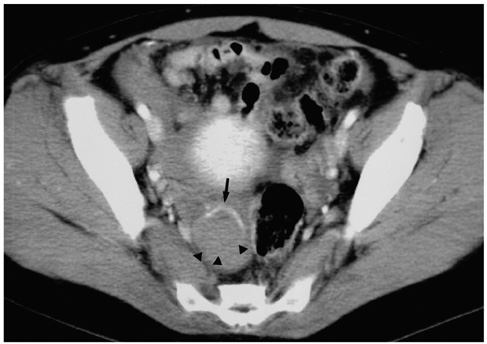
Fig. 1 A 32-year-old woman with severe pelvic pain and a negative pregnancy test. Contrast-enhanced CT scan at the level of the pelvis shows a cystic mass in the right adnexa, with wall enhancement (arrow). There is interruption of the enhancing wall, suggesting rupture of cyst (arrowheads). Note the presence of high-attenuated peritoneal fluid and cystic content.
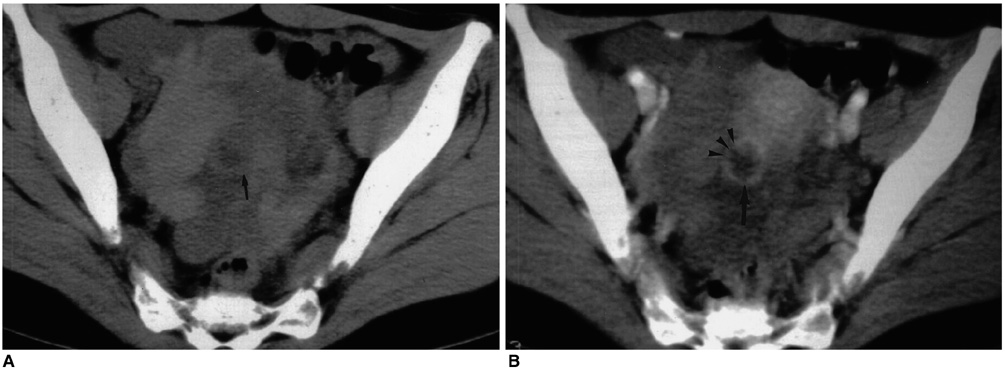
Fig. 2 A 32-year-old woman with severe pelvic pain and a negative pregnancy test. A. Non-enhanced CT scan of the pelvis reveals the presence of high-attenuated peritoneal fluid in the pelvic cavity, due to hemoperitoneum. There is a cystic lesion in the right adnexa (arrow). B. Contrast-enhanced CT shows that the thick wall of the cystic mass (arrow) is well enhanced, interruption is apparent (arrowheads).
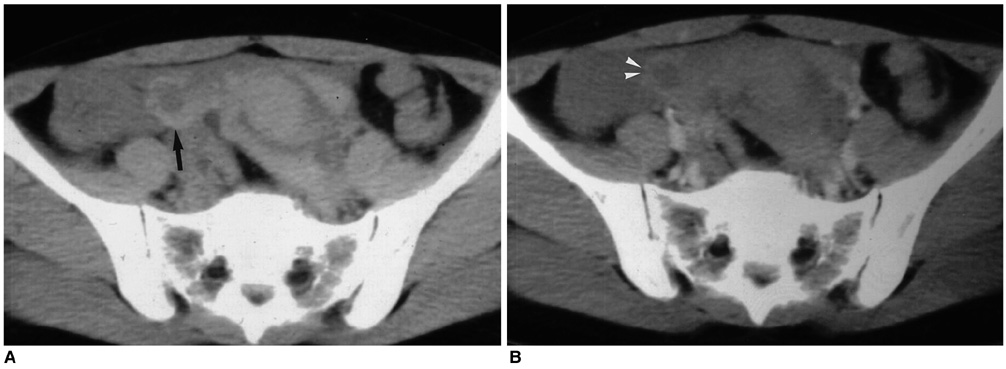
Fig. 3 A 34-year-old woman with lower abdominal pain and anemia. A. Non-enhanced CT scan of the pelvis shows high-attenuated pelvic fluid, suggesting hemoperitoneum. The right adnexa contains a cystic lesion (arrow). B. Contrast-enhanced CT shows that the wall of the right adnexal lesion is well enhanced. In the cystic wall, suspicious interruptions (arrowheads) are apparent.

Fig. 4 A 19-year-old woman with severe pelvic pain and a negative pregnancy test. At contrast-enhanced CT, the wall of the cystic mass (arrow) is well enhanced. Note the presence of high-attenuated fluid in the cul-de sac and dependent portion of the cyst.
Cited by 1 articles
-
Ruptured Corpus Luteal Cyst: Prediction of Clinical Outcomes with CT
Myoung Seok Lee, Min Hoan Moon, Hyunsik Woo, Chang Kyu Sung, Hye Won Jeon, Taek Sang Lee
Korean J Radiol. 2017;18(4):607-614. doi: 10.3348/kjr.2017.18.4.607.
Reference
-
1. Raziel A, Ron-El R, Pansky M, Arieli S, Bukovsky I, Caspi E. Current management of ruptured corpus luteum. Eur J Obstet Gynecol Reprod Biol. 1993. 50:77–81.2. Freistadt H. Ruptured corpus luteum with hemoperitoneum. Am J Obstet Gynecol. 1985. 151:420–421.3. Fraley DS, Johnston JR, Bruns FJ, Adler S, Segel DP. Rupture of ovarian cyst: massive hemoperitoneum in continuous ambulatory peritoneal dialysis patients: diagnosis and treatment. Am J Kidney Dis. 1988. 12:69–71.4. Sarihan H, Unal M, Ozoran Y. Massive haemoperitoneum due to spontaneous rupture of ovarian cyst in children. A report of two cases. S Afr J Surg. 1996. 34:44–46.5. Nyberg DA, Porter BA, Olds MO, et al. MR imaging of hemorrhagic adnexal masses. J Comput Assist Tomogr. 1987. 11:664–669.6. Baltarowich OH, Kurtz AB, Pasto ME, Rifkin MD, Needleman L, Goldberg BB. The spectrum of sonographic findings in hemorrhagic ovarian cysts. AJR Am J Roentgenol. 1987. 148:901–905.7. Bass IS, Haller JO, Friedman AP, Twersky J, Balsam D, Gottesman R. The sonographic appearance of the hemorrhagic ovarian cyst in adolescents. J Ultrasound Med. 1984. 3:509–513.8. Hertzberg BS, Kliewer MA, Paulson EK. Ovarian cyst rupture causing hemoperitoneum: imaging features and the potential for misdiagnosis. Abdom Imaging. 1999. 24:304–308.9. Wilbur AC, Goldstein LD, Prywitch BA. Hemorrhagic ovarian cysts in patients on anticoagulation therapy: CT findings. J Comput Assist Tomogr. 1993. 17:623–625.10. Droegemueller W. Benign gynecologic lesions: Comprehensive gynecology. 1992. St. Louis: Mosby Year Book;521–526.11. Fleischer AC, Javitt MC, Jefferey RB Jr, Jones HW III. Clinical gynecologic imaging. 1997. Philadelphia: Lippincott-Raven Publishers;51–52.12. Reynolds T, Hill MC, Glassman LM. Sonography of hemorrhagic ovarian cysts. J Clin Ultrasound. 1986. 14:449–453.13. Occhipinti KA, Frankel SD, Hricak H. The ovary: computed tomography and magnetic resonance imaging. Radiol Clin North Am. 1993. 31:1115–1132.14. Mitchell DG, Mintz MC, Spritzer CE, et al. Adnexal masses: MR imaging observations at 1.5 T, with US and CT correlation. Radiology. 1987. 162:319–324.15. Fleischer AC, Javitt MC, Jefferey RB Jr, Jones HW III. Clinical gynecologic imaging. 1997. Philadelphia: Lippincott-Raven Publishers;104.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ruptured Corpus Luteal Cyst: Prediction of Clinical Outcomes with CT
- A case of Hyperstimulated Corpus luteal cyst torsion in Pregnancy after In vitro Fertilization
- Corpus Luteum Cyst Rupture - US Findings and Clinical Features
- Agenesis of Corpus Callosum
- Membrane Potential in Luteal Cells from Cyclic Rats: Relationship to Steroidogenic Capacity
