Bronchiolitis Obliterans after Allogenic Bone Marrow Transplantation: HRCT Findings
- Affiliations
-
- 1Department of Radiology, St. Mary's Hospital, College of Medicine, The Catholic University of Korea. jijung@catholic.ac.kr
- 2Catholic Hemopoietic Stem Cell Transplantation Center, College of Medicine, The Catholic University of Korea.
- KMID: 753990
- DOI: http://doi.org/10.3348/kjr.2004.5.2.107
Abstract
OBJECTIVE
To evaluate the high resolution computed tomography (HRCT) findings of bronchiolitis obliterans (BO) after bone marrow transplantation (BMT). MATERIALS AND METHODS: During the past three years, 11 patients were diagnosed as having BO after BMT when they developed irreversible air flow obstruction, with an FEV1 value of less than 80% of the baseline value, without any clinical evidence of infection. All 11 patients underwent HRCT, of whom eight also underwent follow-up HRCT. The HRCT images were assessed retrospectively for the presence of decreased lung attenuation, segmental or subsegmental bronchial dilatation, diminution of peripheral vascularity, centrilobular nodules, and branching linear structure on the inspiratory images. The lobar distribution of the decreased lung attenuation and bronchial dilatation was also examined. The presence of air trapping was investigated on the expiratory images. The interval changes of the HRCT findings were evaluated in those patients who had follow-up images. RESULTS: Abnormal HRCT findings were present in all cases; the most common abnormalities were decreased lung attenuation (n=11), subsegmental bronchial dilatation (n=6), diminution of peripheral vascularity (n=6), centrilobular nodules or branching linear structure (n=3), and segmental bronchial dilatation (n=3). Expiratory air trapping was noted in all patients. The decreased lung attenuation and bronchial dilatations were more frequent or extensive in the lower lobes. Interval changes were found in all patients with follow-up HRCT: increased extent of decreased lung attenuation (n=7) ; newly developed or progressed bronchial dilatation (n=4) ; and increased lung volume (n=3). CONCLUSION: HRCT scans are abnormal in patients with BO, with the most commonly observed finding being areas of decreased lung attenuation. While the HRCT findings are not specific, it is believed that their common features can assist in the diagnosis of BO in BMT recipients.
Keyword
MeSH Terms
Figure
-
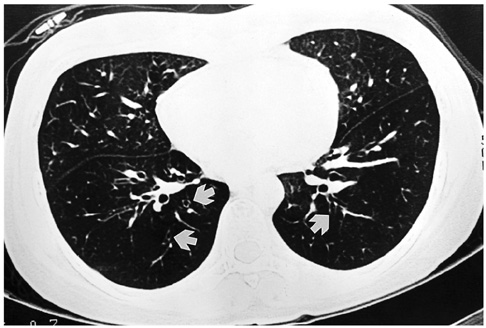
Fig. 1 A 24-year-old woman with bronchiolitis obliterans. She underwent allogeneic bone marrow transplantation for chronic myelocytic leukemia approximately 11 months previously. Inspiratory high resolution computed tomography at the time of diagnosis of bronchiolitis obliterans shows diffuse hypoattenuation and thin-walled dilated bronchi (white arrows) in both lower
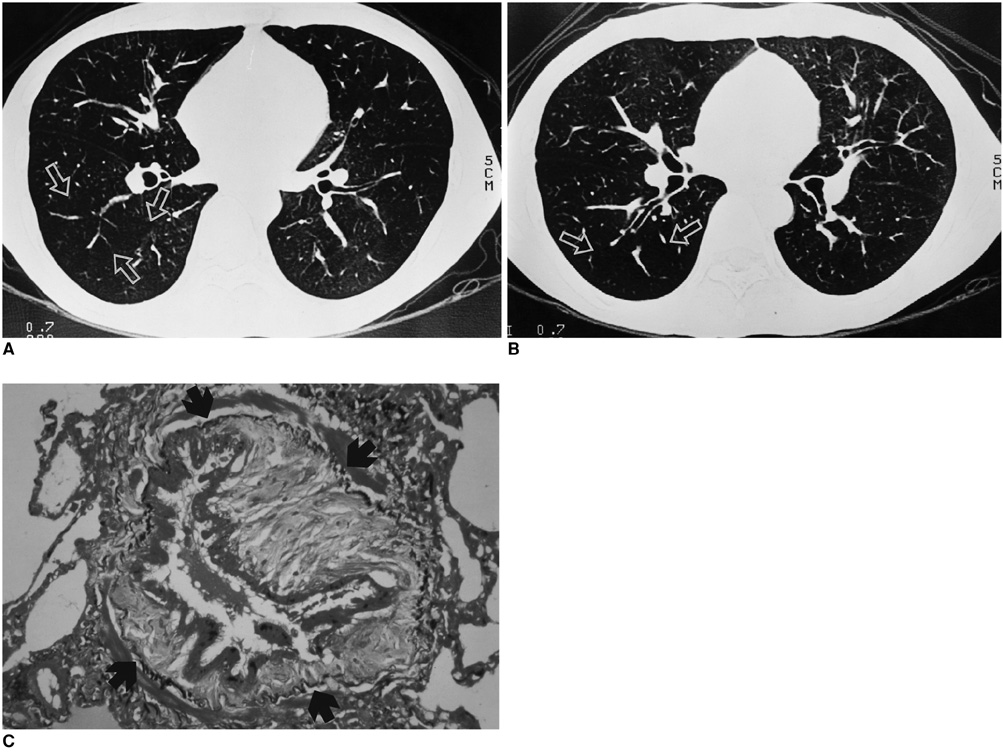
Fig. 2 A 29-year-old man with bronchiolitis obliterans. He underwent allogeneic bone marrow transplantation for chronic myelocytic leukemia approximately one year previously. A. Inspiratory high resolution computed tomography shows diffuse decreased lung attenuation. The pulmonary vessels are sparse and attenuated in the region of decreased density (arrows). B. Expiratory scan shows air trapping within the diseased region (arrows). C. Photomicrograph (elastic van Gieson stain, ×200) shows narrowing of bronchial lumen due to fibrosis of the lamina propria, surrounded by an elastic bundle (arrows) (from Journal of Thoracic Imaging 2001;16:130-37 "notes from 2000 annual meeting of Korean Society of Thoracic Radiology" with permission).

Fig. 3 Tree-in-buds of bronchiolitis obliterans in a 28-year-old woman. Bronchiolitis obliterans was diagnosed on spirometry and transbronchial lung biopsy 16 months after bone marrow transplantation for chronic myelocytic leukemia. Inspiratory high resolution computed tomography scan shows decreased lung attenuation and subsegmental bronchial dilatations in left lower lobe. Tree-in-bud pattern is noted in subpleural portion of posterior basal segment of left lower lobe (arrow).

Fig. 4 Progression of bronchiolitis obliterans on high resolution computed tomography in a 28-year-old woman. Bronchiolitis obliterans was diagnosed on spirometry and transbronchial lung biopsy 16 months after bone marrow transplantation for chronic myelocytic leukemia. A. Inspiratory high resolution computed tomography scan at the time of diagnosis of bronchiolitis obliterans shows small areas of decreased lung attenuation in both upper lobes (arrows). B. Inspiratory high resolution computed tomography scan taken nine months later at a similar anatomic level to A, shows markedly increased extent of pulmonary hypoattenuation and new development of subsegmental bronchial dilatations. The lung volume is much increased.
Cited by 1 articles
-
Risk Factor and Clinical Outcome of Bronchiolitis Obliterans Syndrome after Allogeneic Hematopoietic Stem Cell Transplantation
Chin Kook Rhee, Jick Hwan Ha, Jae Ho Yoon, Byung Sik Cho, Woo-Sung Min, Hyoung Kyu Yoon, Jong Wook Lee
Yonsei Med J. 2016;57(2):365-372. doi: 10.3349/ymj.2016.57.2.365.
Reference
-
1. Epler GR, Colby TV. The spectrum of bronchiolitis obliterans. Chest. 1983. 83:161–162.2. Ezri T, Kunichezky S, Eliraz A, Soroker D, Halperin D, Schattner A. Bronchiolitis obliterans-current concepts. Q J Med. 1994. 87:1–10.3. Roca J, Granena A, Rodriguez-Rosin R, Alvarez P, Agusti-Vidal A, Rozman C. Fatal airways disease in an adult with chronic graft-versus-host disease. Thorax. 1982. 37:77–78.4. Holland HK, Wingard JR, Beschorner WE, Saral R, Santos GW. Bronchiolitis obliterans in bone marrow transplantation and its relationship to chronic graft-v-host disease and low serum IgG. Blood. 1998. 72:621–627.5. Epler GR. Bronchiolitis obliterans and airways obstruction associated with graft-versus-host disease after bone marrow transplantation. Thorax. 1984. 39:887–894.6. Clark JG, Crawford SW, Madtes DK, Sullivan KM. Obstruction lung disease after allogeneic bone marrow transplantation. Clinical presentation and course. Ann Intern Med. 1989. 111:368–376.7. Ralph DD, Springmeyer SC, Sullivan KM, Hackman RC, Storb R, Thomas ED. Rapidly progressive air-flow obstruction in marrow transplant recipients. Possible association between obliterative bronchiolitis and chronic graft-versus-host disease. Am Rev Respir Dis. 1984. 129:641–644.8. Schultz KR, Green GJ, Wensley D, et al. Obstructive lung disease in children after allogeneic bone marrow transplantation. Blood. 1994. 84:3212–3220.9. Sargent MA, Cairns RA, Murdoch MJ, Nadel HR, Wensley D, Schultz KR. Obstructive lung disease in children after allogeneic bone marrow transplantation: evaluation with high-resolution CT. AJR Am J Roentgenol. 1995. 164:693–696.10. Paradis I, Yousem S, Griffith B. Airway obstruction and bronchiolitis obliterans after lung transplantation. Clin Chest Med. 1993. 14:751–763.11. Lentz D, Bergin CJ, Berry GJ, Stoehr C, Theodore J. Diagnosis of bronchiolitis obliterans in heart-lung transplant patients: importance of bronchial dilatation on CT. AJR Am J Roentgenol. 1992. 159:463–467.12. Morrish WF, Herman SJ, Weisbrod GL, Chamberlain DW. Bronchiolitis obliterans after lung transplantation: findings at chest radiography and high-resolution CT. Toronto Lung Transplant Group. Radiology. 1991. 179:487–490.13. Herman SJ. Radiologic assessment after lung transplantation. Clin Chest Med. 1990. 11:333–346.14. Skeens JL, Fuhrman CR, Yousem SA. Bronchiolitis obliterans in heart-lung transplantation patients: radiologic findings in 11 patients. AJR Am J Roentgenol. 1989. 153:253–256.15. Ikonen T, Kivisaari L, Taskinen E, Piilonen A, Harjula AL. High-resolution CT in long-term follow-up after lung transplantation. Chest. 1997. 111:370–376.16. Leung AN, Fisher K, Valentine V, et al. Bronchiolitis obliterans after lung transplantation: detection using expiratory HRCT. Chest. 1998. 113:365–370.17. Bankier AA, Van Muylem AV, Knoop C, Estenne M, Gevenois PA. Bronchiolitis obliterans syndrome in heart-lung transplant recipients: diagnosis with expiratory CT. Radiology. 2001. 218:533–539.18. Ooi GC, Peh WCG, Ip M. High-resolution computed tomography of bronchiolitis obliterans syndrome after bone marrow transplantation. Respiration. 1998. 65:187–191.19. Cooper JD, Billingham M, Egan T, et al. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allograft. International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 1993. 12:713–716.20. Webb WR, Müller NL, Naidich DP. High-resolution CT of the lung. 2001. 3rd ed. Philadelphia: Williams & Wilkins;599–618.21. Chan CK, Hyland RH, Hutcheon MA, et al. Small-airways disease in recipients of allogeneic bone marrow transplants. An analysis of 11 cases and a review of the literature. Medicine. 1987. 66:327–340.22. Krowka MJ, Rosenow EC III, Hoagland HC. Pulmonary complications of bone marrow transplantation. Chest. 1985. 87:237–246.23. Paz HL, Crilley P, Topolsky DC, Coll WX, Patchefsky A, Brodsky I. Bronchiolitis obliterans after bone marrow transplantation: the effect of preconditioning. Respiration. 1993. 60:109–114.24. Theodore J, Starnes VA, Lewiston NJ. Obliterative bronchiolitis. Clin Chest Med. 1990. 11:309–321.25. Philit F, Wiesendanger T, Archimbaud E, Mornex JF, Brune J, Cordier JF. Post-transplant obstructive lung disease ("bronchiolitis obliterans") a clinical comparative study of bone marrow and lung transplant patients. Eur Respir J. 1995. 8:551–558.26. Curtis DJ, Smale A, Thien F, Schwarer AP, Szer J. Chronic airflow obstruction in long-term survivors of allogeneic bone marrow transplantation. Bone Marrow Transplant. 1995. 16:169–173.27. King TE Jr. Bronchiolitis obliterans. Lung. 1989. 167:69–93.28. McLoud TC, Epler GR, Colby TV, Gaensler EA, Carrington CB. Bronchiolitis obliterans. Radiology. 1986. 159:1–8.29. Padley SP, Adler BD, Hansell M, Müller NL. Bronchiolitis obliterans: high-resolution CT findings and correlation with pulmonary function tests. Clin Radiol. 1993. 47:236–240.30. Hruban RH, Ren H, Kuhlman JE, et al. Inflation-fixed lungs: Pathologic-radiologic (CT) correlation of lung transplantation. J Comput Assist Tomogr. 1990. 14:329–335.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent Pneumomediastinum and Subcutaneous Emphysema Complicating Chronic Graft versus Host Disease after Allogeneic Bone Marrow Transplantation
- Recurrent Secondary Pneumothorax Caused by Bronchiolitis Obliterans Due to Chronic Graft Versus Host Disease in a Patient with Chronic Myelogenous Leukemia after Allogenic Bone Marrow Transplantation
- Bronchiolitis obliterans in renal transplant patients
- Pumpless extracorporeal interventional lung assist for bronchiolitis obliterans after allogenic peripheral blood stem cell transplantation for acute lymphocytic leukemia
- A case of bronchiolitis obliterans with bronchiectasis
