Vidian Nerve Schwannoma Extending Into the Foramen Rotundum in a Female Patient: A Case Report
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Kyung Hee University Hospital at Gangdong, Kyung Hee University College of Medicine, Seoul, Republic of Korea
- KMID: 2561503
- DOI: http://doi.org/10.18787/jr.2024.00028
Abstract
- Schwannomas are benign tumors that can develop in any part of a nerve containing Schwann cells. Skull base schwannomas are rare, representing approximately 4% of extracranial schwannomas. Among these, vidian nerve schwannomas are particularly uncommon, with only a few documented cases. In this report, we describe the case of a 58-year-old female patient who presented with an incidental finding of a skull base mass. The patient’s only symptoms were intermittent headaches and dry eyes. No mass was detected during the physical examination. Radiographic evaluation revealed a neoplasm within the vidian canal, and the lesion’s characteristics suggested a schwannoma. The patient underwent endoscopic resection, and subsequent histopathological analysis confirmed the diagnosis of schwannoma. Follow-up imaging and physical examination showed no evidence of recurrence. This case report highlights a schwannoma located in the vidian canal and extending into the foramen rotundum, which was successfully managed with endoscopic surgery.
Figure
-
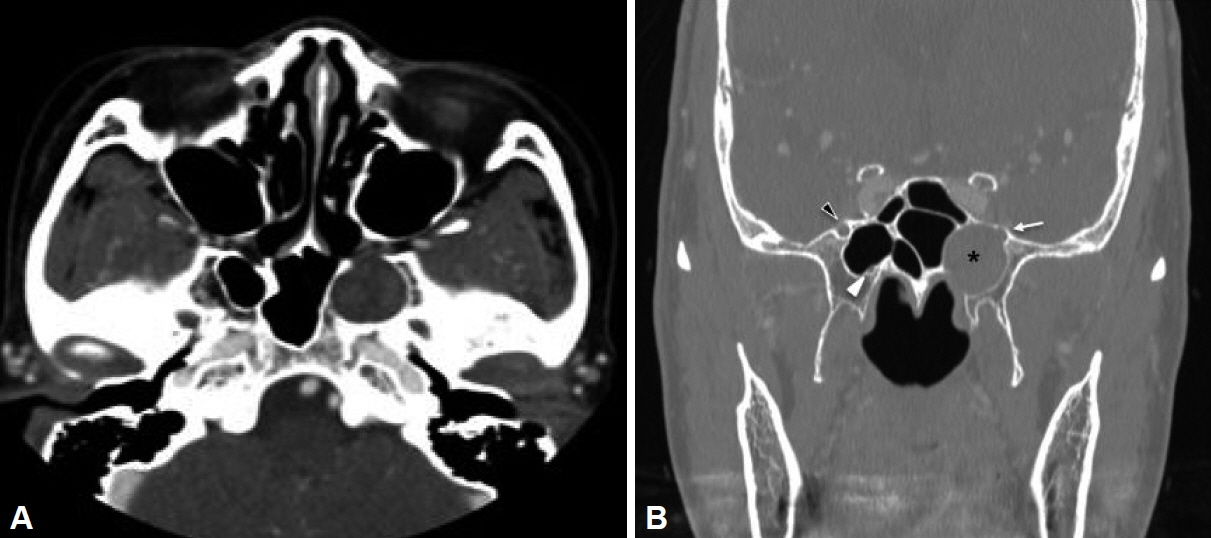
Fig. 1. Axial and coronal views of a computed tomography scan of the paranasal sinus. A: A round mass is observed within the vidian canal, extending into the left sphenoid sinus. The pterygopalatine fossa remains intact. B: A soft tissue density mass-like lesion (asterisk) occupies the vidian canal, extending into the sphenoid sinus and foramen rotundum. The medial wall of the foramen rotundum’s bony canal is partially eroded. White arrowhead: right vidian canal. Black arrowhead: right foramen rotundum. White arrow: left foramen rotundum, showing destruction of the bony canal.

Fig. 2. Preoperative axial and coronal magnetic resonance image. A: A hypermetabolic lesion exhibiting a heterogeneously enhanced “salt and pepper” sign is observed on a T1-weighted axial image. B: The left maxillary nerve is not observed on the T1-weighted coronal image, in contrast to the foramen rotundum on the right side (white arrowhead).
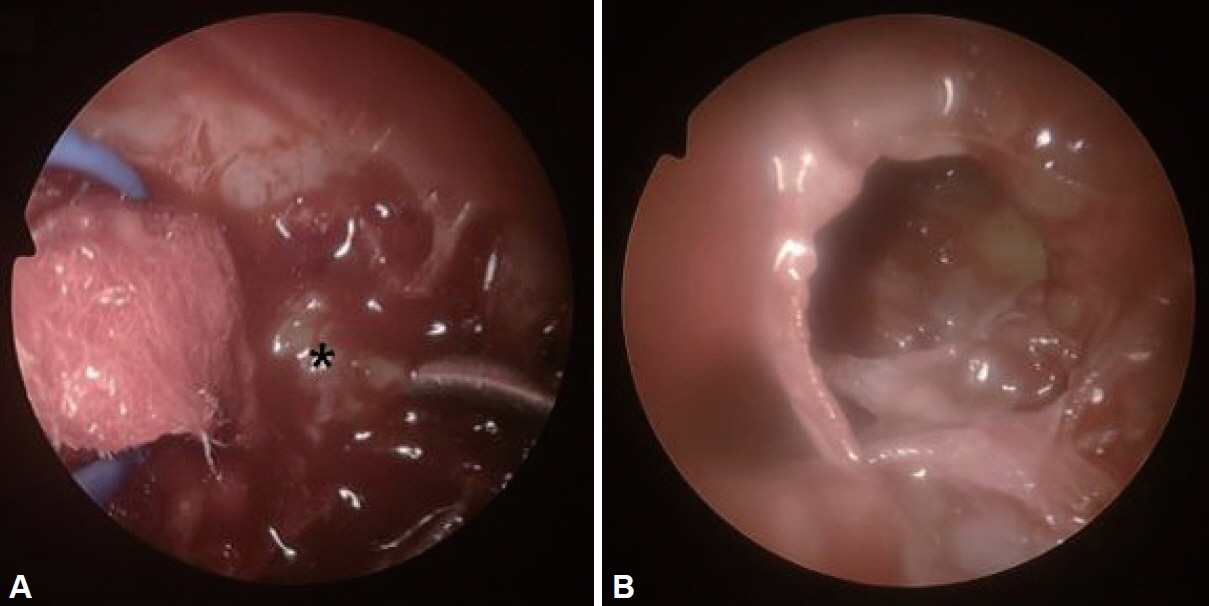
Fig. 3. Intraoperative image of schwannoma. A: A round mass containing yellowish tissue (asterisk) is visible. Intracapsular piecemeal resection was performed using the appropriate equipment. B: All intracapsular components were removed and confirmed with a 30° endoscope.

Fig. 4. Histopathologic findings of the mass. A: Verocay body arranged in a palisading pattern with compact areas of spindle cells, representing the Antoni A area, alongside loosely arranged hypocellular foci in the Antoni B area (hematoxylin & eosin stain, ×100). B: Immunohistochemical staining yielded a strongly positive reaction for S-100 protein, a useful marker for schwannoma (S-100 stain, ×100).
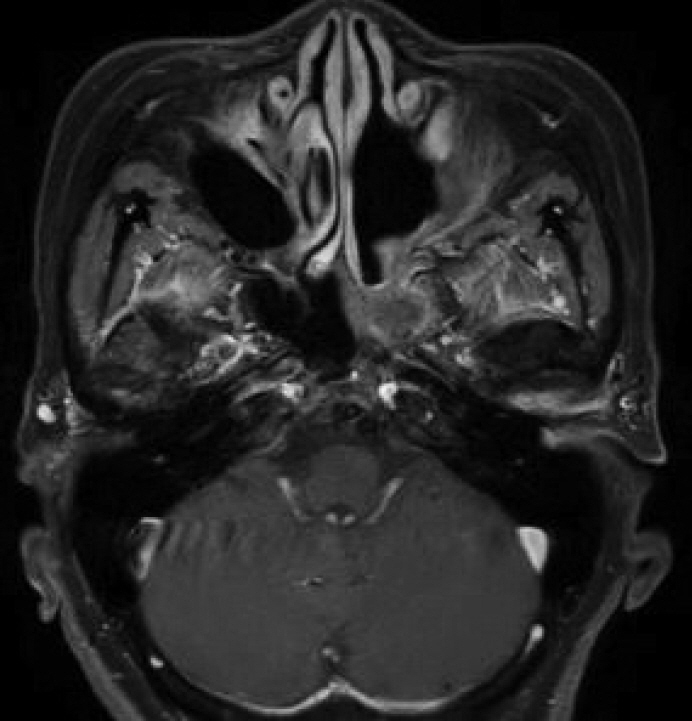
Fig. 5. Postoperative magnetic resonance T1-weighted image showing no evidence of recurrence in the area of the vidian canal, with associated mucosal swelling.
Reference
-
References
1. Buob D, Wacrenier A, Chevalier D, Aubert S, Quinchon JF, Gosselin B, et al. Schwannoma of the sinonasal tract: a clinicopathologic and immunohistochemical study of 5 cases. Arch Pathol Lab Med. 2003; 127(9):1196–9.
Article2. Verma P, Riju J, Ramalingam N, Zeinuddeen R, Paulose AA, Susheel S, et al. Extracranial head and neck schwannomas: a single centre retrospective experience of 97 cases. Indian J Otolaryngol Head Neck Surg. 2024; 76(5):4292–9.
Article3. Lee JC, Kao CH, Hsu CH, Lin YS. Endoscopic transsphenoidal vidian neurectomy. Eur Arch Otorhinolaryngol. 2011; 268(6):851–6.
Article4. Honda K, Asato R, Tanaka S, Endo T, Nishimura K, Ito J. Vidian nerve schwannoma with middle cranial fossa extension resected via a maxillary swing approach. Head Neck. 2008; 30(10):1389–93.
Article5. Masroor FA, Gilde J, Liang J. Vidian nerve schwannoma: a rare skullbase neoplasm presenting with ocular manifestations: a case report and literature review. Perm J. 2018; 22:18–021.
Article6. Hackman T, Rickert CG, Getz AE, Uppaluri R. Endoscopic surgical management of vidian nerve schwannoma. Laryngoscope. 2011; 121(2):241–4.
Article7. Yamasaki A, Sedaghat AR, Lin GC, Curry WT, Shih HA, Gray ST. A rare finding of schwannoma of the vidian canal: a case report. J Neurol Surg Rep. 2015; 76(1):e48–51.
Article8. Bidarkotimath S, Viveka S, Udyavar A. Vidian canal: radiological anatomy and functional correlations. J Morphol Sci. 2017; 29(1):27–31.9. McLaughlin N, Bresson D, Ditzel Filho LF, Carrau RL, Kelly DF, Prevedello DM, et al. Vidian nerve neurofibroma removed via a transpterygoid approach. Minim Invasive Neurosurg. 2011; 54(5-6):250–2.10. Peridis S, Moonim MT, Roberts D, Al-Sarraj S, Hopkins C. Desmoplastic fibroma of the vidian canal in a child: case report. J Laryngol Otol. 2011; 125(7):753–6.11. Tanaka C, Kikuchi M, Matsunaga M, Omori K, Nakagawa T. Endoscopic endonasal surgery of a large vidian nerve schwannoma with preparation for avoiding major vascular injury. Cureus. 2021; 13(3):e14230.
Article12. Kim YS, Kim HJ, Kim CH, Kim J. CT and MR imaging findings of sinonasal schwannoma: a review of 12 cases. AJNR Am J Neuroradiol. 2013; 34(3):628–33.13. Niepel AL, Steinkellner L, Sokullu F, Hellekes D, Kömürcü F. Long-term follow-up of intracapsular schwannoma excision. Ann Plast Surg. 2019; 82(3):296–8.14. Pasic TR, Makielski K. Nasal schwannoma. Otolaryngol Head Neck Surg. 1990; 103(6):943–6.
Article15. Neville BW, Damm DD, Allen CM, Bouquot JE. Soft tissue tumors. In: Oral and maxillofacial pathology. 3rd ed. St. Louis (MO): Elsevier; 2009. p.507-70.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Vidian Nerve Schwannoma: Resection by Endoscopic Sinus Surgery
- Endoscopic Transnasal Vidian Neurectomy for Intractable Allergic Rhinitis
- A Case of Large Foramen Magnum Schwannoma
- A Case of Jacobson's Nerve Schwannoma Extending into the External Auditory Canal
- A Case of Facial Nerve Schwannoma Extending into the Middle Cranial Fossa
