Primary epithelioid inflammatory myofibroblastic sarcoma of the brain with EML4::ALK fusion mimicking intra-axial glioma: a case report and brief literature review
- Affiliations
-
- 1Departments of Pathology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 2Departments of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 3Departments of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2555540
- DOI: http://doi.org/10.4132/jptm.2024.04.12
Abstract
- An aggressive subtype of inflammatory myofibroblastic tumor, epithelioid inflammatory myofibroblastic sarcoma occurs primarily inside the abdominal cavity, followed by a pulmonary localization. Most harbor anaplastic lymphoma kinase (ALK) gene rearrangements, with RANBP2 and RRBP1 among the well-documented fusion partners. We report the second case of primary epithelioid inflammatory myofibroblastic sarcoma of the brain, with a well-known EML4::ALK fusion. The case is notable for its intra-axial presentation that clinico-radiologically mimicked glioma.
Keyword
Figure
-
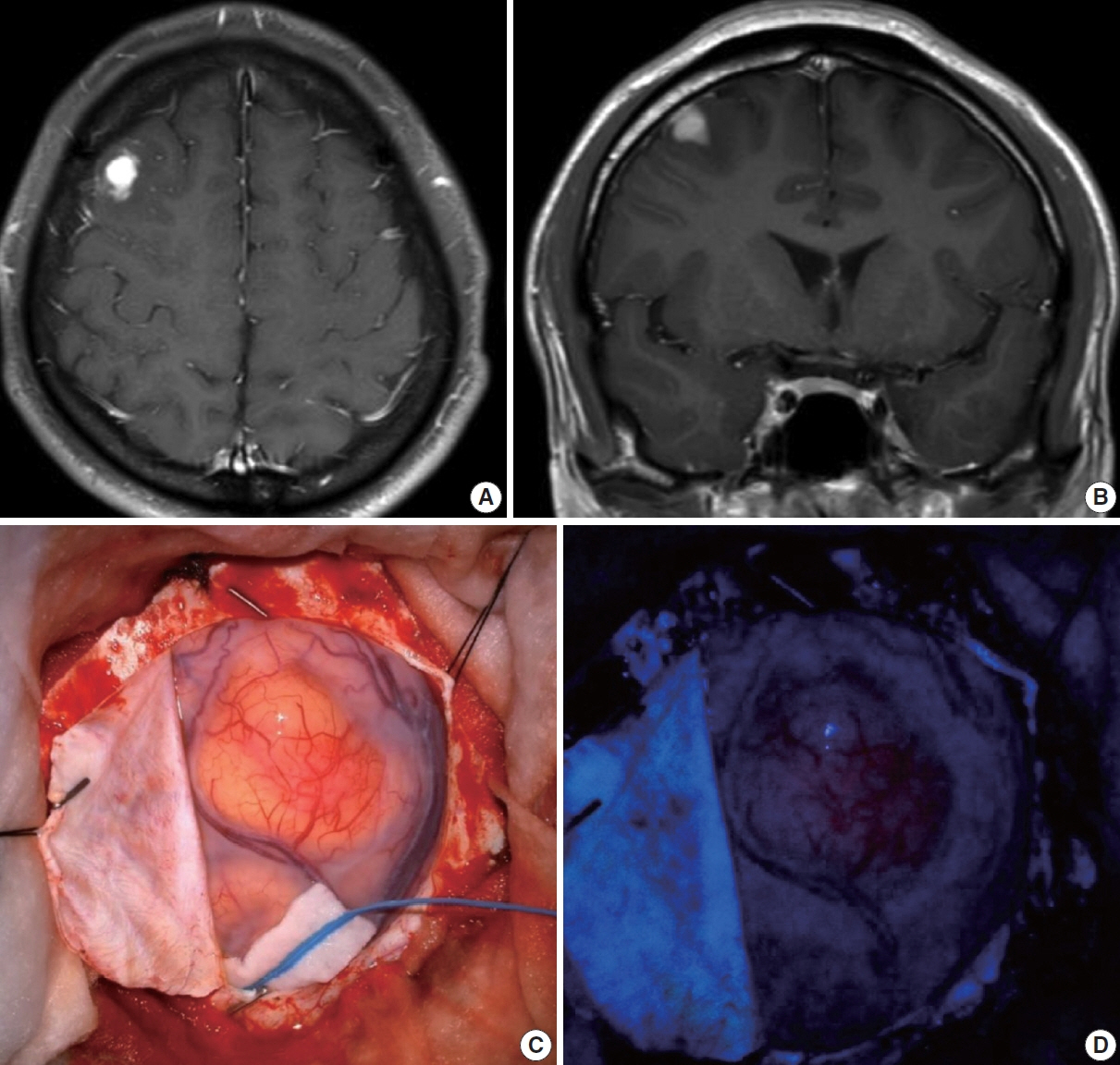
Fig. 1. Contrast-enhanced magnetic resonance imaging (MRI) glioma study (3.0T) and intraoperative surgical field view. T1 axial (A) and coronal (B) preoperative MRI of the 1.5 cm vividly enhancing mass in the right frontal lobe with no intralesional hemorrhage or calcification. (C) Intraoperative surgical field view during the right frontal craniotomy and tumor removal. (D) Intraoperative 5-aminolevulinic acid uptake in the tumor.
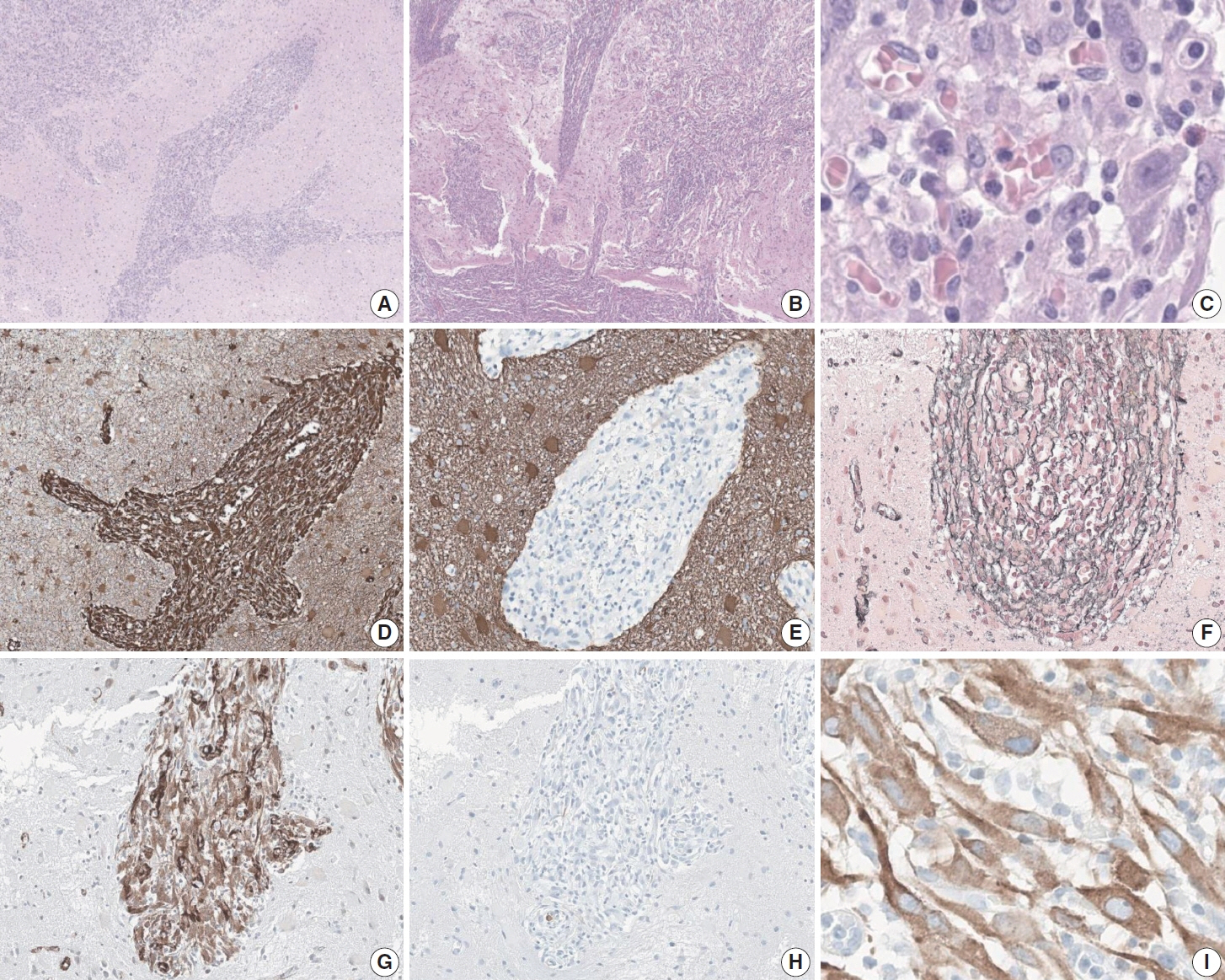
Fig. 2. Histomorphology and immunophenotype of primary epithelioid inflammatory myofibroblastic sarcoma (EIMS) in the brain. (A) At low power, the perivascular infiltration of the tumor is apparent. (B) Low power also illustrates the appearance of the tumor to extend from the pia mater (lower left) into the brain parenchyme. (C) At high-power, perivascular growth is still observed, with lymphoplasmacytic infiltrate. EIMS tumor cells have low nuclear-cytoplasmic ratio, owing to their plump cytoplasm, but the absolute size of their nuclei are 3–4 times larger than that of vascular endothelial cells, with some tumor nucleoli the size of nearby lymphocyte nuclei. Vimentin immunohistochemical (IHC) stain was strong and diffuse positive (D), while glial fibrillary acidic protein IHC stain was totally negative (E). (F) Reticulin special stain was negative in the tumor and positive in the stroma. Smooth muscle actin IHC stain was positive (G), while desmin IHC stain was negative (H). (I) Anaplastic lymphoma kinase IHC stain with the 5A4 clone showed the characteristic perinuclear staining.
Reference
-
References
1. Marino-Enriquez A, Wang WL, Roy A, et al. Epithelioid inflammatory myofibroblastic sarcoma: an aggressive intra-abdominal variant of inflammatory myofibroblastic tumor with nuclear membrane or perinuclear ALK. Am J Surg Pathol. 2011; 35:135–44.2. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor): a clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol. 1995; 19:859–72.
Article3. Gleason BC, Hornick JL. Inflammatory myofibroblastic tumours: where are we now? J Clin Pathol. 2008; 61:428–37.
Article4. Chopra S, Maloney N, Wang WL. Epithelioid inflammatory myofibroblastic sarcoma with VCL-ALK fusion of central nervous system: case report and brief review of the literature. Brain Tumor Pathol. 2022; 39:35–42.
Article5. WHO Classification of Tumors Editorial Board. WHO classification of tumours: central nervous system tumours. 5th ed. Lyon: International Agency for Research on Cancer;2021.6. Yu L, Liu J, Lao IW, Luo Z, Wang J. Epithelioid inflammatory myofibroblastic sarcoma: a clinicopathological, immunohistochemical and molecular cytogenetic analysis of five additional cases and review of the literature. Diagn Pathol. 2016; 11:67.
Article7. Lee JC, Li CF, Huang HY, et al. ALK oncoproteins in atypical inflammatory myofibroblastic tumours: novel RRBP1-ALK fusions in epithelioid inflammatory myofibroblastic sarcoma. J Pathol. 2017; 241:316–23.
Article8. Singh P, Nambirajan A, Gaur MK, et al. Primary pulmonary epithelioid inflammatory myofibroblastic sarcoma: a rare entity and a literature review. J Pathol Transl Med. 2022; 56:231–7.
Article9. Yamamoto H, Yoshida A, Taguchi K, et al. ALK, ROS1 and NTRK3 gene rearrangements in inflammatory myofibroblastic tumours. Histopathology. 2016; 69:72–83.
Article10. Drilon A, Laetsch TW, Kummar S, et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N Engl J Med. 2018; 378:731–9.11. Lovly CM, Gupta A, Lipson D, et al. Inflammatory myofibroblastic tumors harbor multiple potentially actionable kinase fusions. Cancer Discov. 2014; 4:889–95.
Article12. Sokai A, Enaka M, Sokai R, et al. Pulmonary inflammatory myofibroblastic tumor harboring EML4-ALK fusion gene. Jpn J Clin Oncol. 2014; 44:93–6.
Article13. Jiang Q, Tong HX, Hou YY, et al. Identification of EML4-ALK as an alternative fusion gene in epithelioid inflammatory myofibroblastic sarcoma. Orphanet J Rare Dis. 2017; 12:97.
Article14. Fletcher CD, Bridge JA, Hogendoorn PC, Mertens F. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon: IARC Press;2013.15. WHO Classification of Tumors Editorial Board. WHO classification of tumours: breast tumours. 5th ed. Lyon: International Agency for Research on Cancer;2019.16. Zhou L, Pan W, Huang R, Lu Z, You Z, Li Y. Intracranial inflammatory myofibroblastic tumor: a literature review and a rare case misdiagnosed as acoustic neuroma. Diagnostics (Basel). 2023; 13:2725.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary pulmonary epithelioid inflammatory myofibroblastic sarcoma: a rare entity and a literature review
- A case of epithelioid sarcoma arising in the vulva
- EML4-ALK Fusion Gene in Korean Non-Small Cell Lung Cancer
- A Case of Simultaneously Diagnosed Lung Adenocarcinoma and Endobronchial Inflammatory Myofibroblastic Tumor with Two Distinct Types of ALK Translocation
- A Case of Epithelioid Sarcoma in a Child
