J Rhinol.
2024 Mar;31(1):46-51. 10.18787/jr.2023.00072.
Internal Carotid Artery Pseudoaneurysm in a Patient Presenting With Recurrent Epistaxis: A Case Report and Literature Review
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Chosun University College of Medicine, Gwangju, Republic of Korea
- KMID: 2554091
- DOI: http://doi.org/10.18787/jr.2023.00072
Abstract
- Traumatic pseudoaneurysms are uncommon vascular lesions that can result from traumatic injuries to the nasal and facial areas. They pose a significant clinical challenge due to their potential to cause recurrent and life-threatening epistaxis. Understanding the underlying vascular anatomy, causes, and treatment options is essential for optimizing patient outcomes. In this case report, we present a 55-year-old man who developed a traumatic pseudoaneurysm of the sphenoid sinus, arising from the cavernous segment of the internal carotid artery following a traumatic incident. This case was successfully managed with stent-assisted coil embolization.
Keyword
Figure
-

Fig. 1. Intraoperative endoscopic images. A: Sphenoid sinus opening. B: A soft tissue mass with pulsation, suspicious for a pseudoaneurysm, was seen inside the sphenoid sinus.

Fig. 2. Computed tomography angiography findings revealed a pseudoaneurysm arising from the cavernous segment of the internal carotid artery in proximity to the site of trauma (arrow).
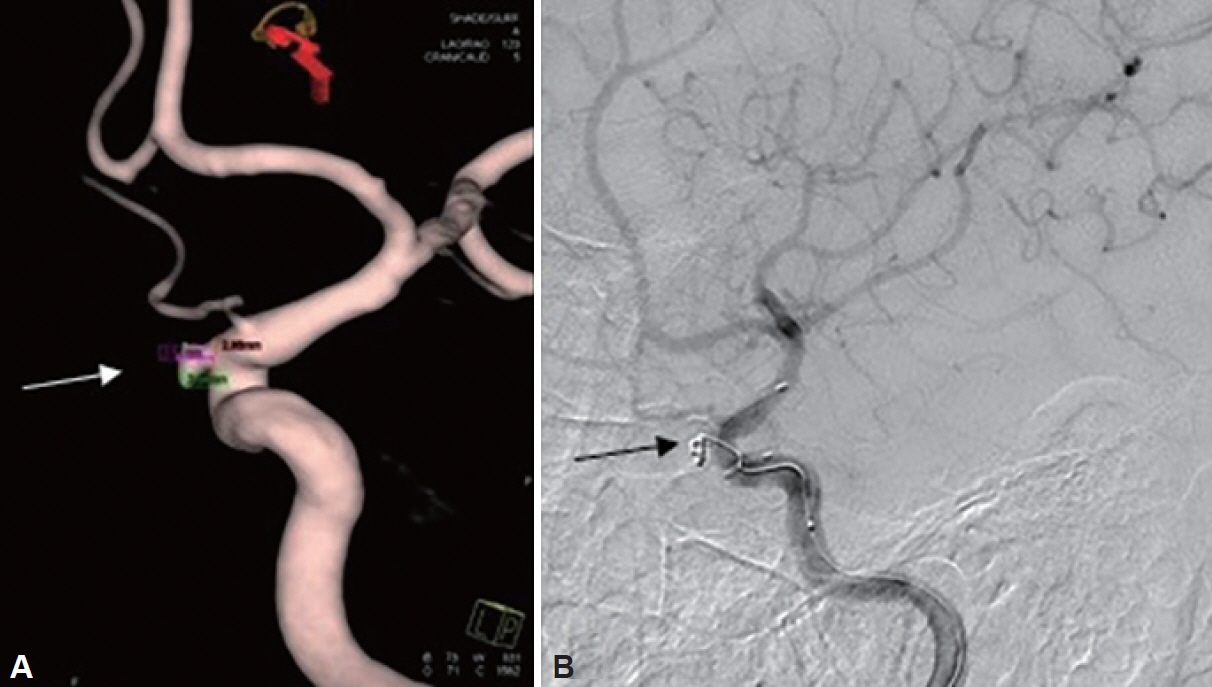
Fig. 3. Stent-assisted coil embolization of the sphenopalatine artery pseudoaneurysm (arrow in A and B). A: 3D computed tomography angiography. B: Digital subtraction angiography.

Fig. 4. After surgery, the coil (arrow) was located in the posterior wall of the sphenoid sinus.
Reference
-
References
1. El Naamani K, Capone S, Chen CJ, Tartaglino L, Rosen M, Abbas R, et al. Sphenopalatine artery pseudoaneurysm formation following facial trauma: a case report and literature review. Interdiscip Neurosurg. 2023; 32:101741.
Article2. Chun JJ, Choi CY, Wee SY, Song WJ, Jeong HG. Embolization for treating posttraumatic pseudoaneurysm of the sphenopalatine artery. Arch Craniofac Surg. 2019; 20(4):251–4.
Article3. O’Brien D Jr, O’Dell MW, Eversol A. Delayed traumatic cerebral aneurysm after brain injury. Arch Phys Med Rehabil. 1997; 78(8):883–5.
Article4. Cohen S, Anastassov GE, Chuang SK. Posttraumatic pseudoaneurysm of the sphenopalatine artery presenting as persistent epistaxis: diagnosis and management. J Trauma. 1999; 47(2):396–9.5. Gökdoğan O, Kizil Y, Aydil U, Karamert R, Uslu S, Ileri F. Sphenopalatine artery pseudoaneurysm: a rare cause of intractable epistaxis after endoscopic sinus surgery. J Craniofac Surg. 2014; 25(2):539–41.6. Deng D, Du J, Liu F, Zhong B, Qiao Y, Liu Y. Clinical characteristics of internal carotid artery pseudoaneurysms in the sphenoid sinus. Am J Otolaryngol. 2019; 40(1):106–9.
Article7. Pelliccia P, Bartolomeo M, Iannetti G, Bonafé A, Makeieff M. Traumatic intra-sphenoidal pseudoaneurysm lodged inside the fractured sphenoidal sinus. Acta Otorhinolaryngol Ital. 2016; 36(2):149–52.8. Fujii K, Chambers SM, Rhoton AL Jr. Neurovascular relationships of the sphenoid sinus. A microsurgical study. J Neurosurg. 1979; 50(1):31–9.9. Chen D, Concus AP, Halbach VV, Cheung SW. Epistaxis originating from traumatic pseudoaneurysm of the internal carotid artery: diagnosis and endovascular therapy. Laryngoscope. 1998; 108(3):326–31.
Article10. Ellis JA, Goldstein H, Connolly ES Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012; 32(5):E9.
Article11. Hasegawa H, Inoue T, Tamura A, Saito I. Urgent treatment of severe symptomatic direct carotid cavernous fistula caused by ruptured cavernous internal carotid artery aneurysm using high-flow bypass, proximal ligation, and direct distal clipping: technical case report. Surg Neurol Int. 2014; 5:49.
Article12. Bavinzski G, Killer M, Knosp E, Ferraz-Leite H, Gruber A, Richling B. False aneurysms of the intracavernous carotid artery--report of 7 cases. Acta Neurochir (Wien). 1997; 139(1):37–43.13. Menon G, Hegde A, Nair R. Post-traumatic cavernous carotid pseudoaneurysm with delayed epistaxis. Cureus. 2018; 10(7):e3002.
Article14. Matos LEO, Cunha JPP, Monteiro MBC, Rodrigues Filho JA, da Ponte KF, Conrado FM, et al. Internal carotid artery pseudoaneurysm as a cause of epistaxis: case-based update. J Bras Neurocirur. 2022; 33(2):245–50.
Article15. Hern JD, Coley SC, Hollis LJ, Jayaraj SM. Delayed massive epistaxis due to traumatic intracavernous carotid artery pseudoaneurysm. J Laryngol Otol. 1998; 112(4):396–8.
Article16. Adeel M, Ikram M. Post-traumatic pseudoaneurysm of internal carotid artery: a cause of intractable epistaxis. BMJ Case Rep. 2012; 2012:bcr0220125927.17. Sridharan R, Low SF, Mohd MR, Kew TY. Intracavernous internal carotid artery pseudoaneurysm. Singapore Med J. 2014; 55(10):e165–8.
Article18. Kim JY, Kim YB, Chung J. Recurrent epistaxis from inflamed granulated tissue and an associated pseudoaneurysm of the internal carotid artery: case report. BMC Neurol. 2021; 21(1):215.
Article19. Moon TH, Kim SH, Lee JW, Huh SK. Clinical analysis of traumatic cerebral pseudoaneurysms. Korean J Neurotrauma. 2015; 11(2):124–30.
Article20. Kim YW, Baek MJ, Kim HD, Cho KS. Massive epistaxis due to pseudoaneurysm of the sphenopalatine artery: a rare post-operative complication of orthognathic surgery. J Laryngol Otol. 2013; 127(6):610–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Pseudoaneurysm of the External and Internal Carotid Artery Presenting as Epistaxis: Case Report
- Technical Pitfalls in the Endovascular Treatment of Traumatic Pseudoaneurysm of the Internal Carotid Artery: Case Report
- A case of petrous carotid artery pseudoaneurysm presenting with epistaxis after radiotherapy in a patient with nasopharyngeal cancer
- A Case of Internal Carotid Artery Traumatic Pseudoaneurysm with Epistaxis: Treated with Detachable Balloon Occlusion (DBO) and Detachable Coil
- Endovascualr Treatment for Traumatic Giant Pseudoaneurysm of Internal Carotid Artery
