Usefulness of Lymphocyte Subset Analysis Using Primary Immunodeficiency Orientation Tube Panel: Two Cases with Primary Immunodeficiency Diseases
- Affiliations
-
- 1Department of Laboratory Medicine, Pusan National University Hospital, Busan, Korea
- 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea
- 3Department of Laboratory Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
- 4Department of Pediatrics, Pusan National University Children’s Hospital, Yangsan, Korea
- KMID: 2552726
- DOI: http://doi.org/10.47429/lmo.2023.13.1.53
Abstract
- Primary immunodeficiency diseases (PIDs) are a heterogeneous group of disorders caused by genetic defects in the immune system and exhibit a variety of clinical manifestations, including recurrent infections. Rapid and proper diagnosis is vital for proper therapeutic intervention. Compared to the conventional lymphocyte subset analysis, the standardized Primary Immunodeficiency Orientation Tube (PIDOT) panel has been proposed to provide a more detailed dissection of lymphocyte subsets according to their differentiation and maturation stages. This helps in screening of a suspected PID sample, and to provide quick guidance regarding further course of testing. Here, we report two cases of PID diagnosed by lymphocyte subset analysis using PIDOT panel to establish its usefulness in a clinical laboratory.
Keyword
Figure
-

Fig. 1 Lymphocyte subset analysis of the peripheral blood (Case 1) by flow cytometry using Primary Immunodeficiency Orientation Tube (PIDOT) panel. Patient’s B-cell subsets show strong reduction in CD27 expression including unswitched memory B cells/plasma cells and switched memory B cells. Impaired maturation of post-GC B-cells is a hallmark of common variable immunodeficiency (CVID). (A) After gating lymphocytes on CD45 channel, forward scatter channel (FSC) and side scatter channel (SSC), CD3 and CD19 in combination with TCRγδ were used to define subsets of lymphocytes; T-cells (upper left), B-cells (lower right) and NK cells (lower left). (B) CD16+CD56+ and CD3 markers were used to define NK cells (upper left). (C) The CD3+ T-cells were divided into CD4+ (lower right), CD8+ (upper left) and double negative T-cells (DNT) (lower left). (D) The double negative T-cells were subdivided into two subpopulations according to the expression of TCRγδ; TCRγδ- T-cells (upper left) and TCRγδ+ T-cells (upper right). (E) CD4+ T-cell subsets were subdivided into naïve (CD27+CD45RA+; upper right), central memory/transitional memory (CM/TM; CD27+CD45RA-; upper left), effector memory (EM; CD27-CD45RA-; lower left) and terminally differentiated (TD; CD27-CD45RA+; lower right) CD4+ T-cells. (F) CD8+ T-cell subsets were subdivided into naïve (CD27+CD45RA+; upper right), CM/TM (CD27+CD45RA-; upper left), EM (CD27-CD45RA-; lower left) and TD (CD27-CD45RA+; lower right) CD8+ T-cells. For CD8+ T-cells, one additional subpopulation is defined, effector CD27dim (middle right). (G) Subdivision of the B-cell subset demonstrated pre-germinal center B-cells (Pre-GC; CD27-CD16-CD56-; lower left) and reduced post-germinal center B-cells (Post-GC; CD27+CD16-CD56-; upper left). (H) Pre-GC B-cells were sub-classified into mature naïve B-cells (CD27-smIgM+IgD++; upper right; brown) and transitional/immature B-cells (CD27-smIgM++IgD+; lower right; magenta) by the intensity of surface membrane immunoglobulin (smIg) M and D markers. (I) Likewise, post-GC B-cells were sub-classified into two different subsets based on the expression level of smIgM and smIgD; unswitched memory B cells/plasma cells (MBC/PC; CD27+smIgM+IgD+; upper right) and switched MBC/PC (CD27+smIgM-IgD-; lower left). In this plot, proportion of post-GC cells was generally reduced.
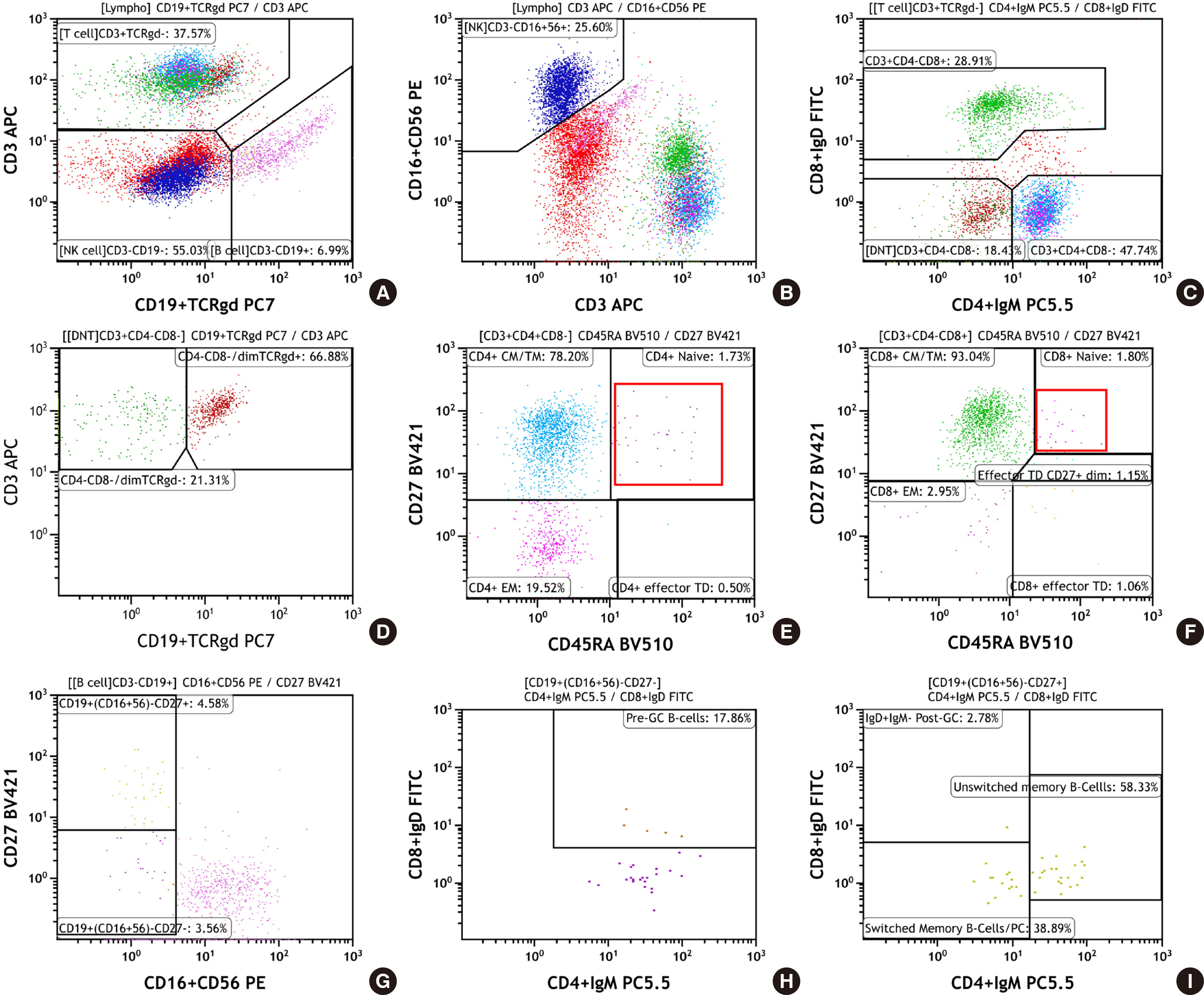
Fig. 2 Lymphocyte subset analysis of the peripheral blood (Case 2) by flow cytometry using Primary Immunodeficiency Orientation Tube (PIDOT) panel. In this patient, naïve CD4+/CD8+ T-cells were markedly reduced along with B-cell subsets, but NK cell population was preserved. (A) After gating lymphocytes on CD45 channel, forward scatter channel (FSC) and side scatter channel (SSC), CD3 and CD19 in combination with TCRγδ were used to define lymphocytes subsets; T-cells (upper left), B-cells (lower right) and NK cells (lower left). (B) CD16+CD56 marker and CD3 marker were used to define NK cells (upper left). (C) The CD3+ T-cells were divided into CD4+, CD8+ and double negative T-cells (DNT). In this plot, the distribution of CD3+ T-cells showed an overall reduction. (D) The double negative T-cells were subdivided into two subpopulations based on the expression of TCRγδ; TCRγδ- T-cells (upper left) and TCRγδ+ T-cells (upper right). (E) CD4+ T-cell subsets were subdivided into naïve (CD27+CD45RA+; upper right), central memory/transitional memory (CM/TM; CD27+CD45RA-; upper left), effector memory (EM; CD27-CD45RA-; lower left) and terminally differentiated (TD; CD27-CD45RA+; lower right) CD4+ T-cells. All CD4+ T-cell subsets were decreased, particularly lack of naïve CD4+ was pronounced. (F) CD8+ T-cell subsets were subdivided into naïve (CD27+CD45RA+; upper right), CM/TM (CD27+CD45RA-; upper left), EM (CD27-CD45RA-; lower left), effector CD27dim (middle right) and TD (CD27-CD45RA+; lower right) CD8+ T-cells. In this case also, there was a decrease in the overall CD8+ T-cell subsets and severe reduction in naïve CD8+ T-cells. (G) Subdivision of the B-cell subsets demonstrated an overall reduction in pre-GC B-cells (CD27-CD16-CD56-; lower left) and post-GC B-cells (CD27+CD16-CD56-; upper left). (H) Reduced pre-GC B-cells were further classified into mature naïve B-cells (CD27-smIgM+IgD++; upper right) and transitional/immature B-cells (CD27-smIgM+IgD+; lower right). (I) Post-GC B-cells were sub-classified into unswitched MBC/PC (CD27+smIgM+IgD+; upper right) and switched MBC/PC (CD27+smIgM-IgD-; lower left).
Reference
-
1. Tangye SG, Al-Herz W, Bousfiha A, Chatila T, Cunningham-Rundles C, Etzioni A, et al. 2020; Human inborn errors of immunity: 2019 update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 40:24–64. DOI: 10.1007/s10875-019-00737-x. PMID: 31953710. PMCID: PMC7082301.2. Abolhassani H, Azizi G, Sharifi L, Yazdani R, Mohsenzadegan M, Delavari S, et al. 2020; Global systematic review of primary immunodeficiency registries. Expert Rev Clin Immunol. 16:717–32. DOI: 10.1080/1744666X.2020.1801422. PMID: 32720819.3. Rhim JW, Kim KH, Kim DS, Kim BS, Kim JS, Kim CH, et al. 2012; Prevalence of primary immunodeficiency in Korea. J Korean Med Sci. 27:788–93. DOI: 10.3346/jkms.2012.27.7.788. PMID: 22787376. PMCID: PMC3390729.4. Leiding JW, Forbes LR. 2019; Mechanism-based precision therapy for the treatment of primary immunodeficiency and primary immunodysregulatory diseases. J Allergy Clin Immunol Pract. 7:761–73. DOI: 10.1016/j.jaip.2018.12.017. PMID: 30832891.5. Aguilar C, Malphettes M, Donadieu J, Chandesris O, Coignard-Biehler H, Catherinot E, et al. 2014; Prevention of infections during primary immunodeficiency. Clin Infect Dis. 59:1462–70. DOI: 10.1093/cid/ciu646. PMID: 25124061.6. Long PM, Sanford KW, Bluth MH. McPherson RA, Pincus MR, editors. 2017. Immunodeficiency disorders. Henry's clinical diagnosis and management by laboratory methods. 23rd ed. p. 984–92. St. Louis, MO: Elsevier.7. Abraham RS, Aubert G. 2016; Flow cytometry, a versatile tool for diagnosis and monitoring of primary immunodeficiencies. Clin Vaccine Immunol. 23:254–71. DOI: 10.1128/CVI.00001-16. PMID: 26912782. PMCID: PMC4820507.8. van der Burg M, Kalina T, Perez-Andres M, Vlkova M, Lopez-Granados E, Blanco E, et al. 2019; The EuroFlow PID Orientation Tube for flow cytometric dDiagnostic screening of primary immunodeficiencies of the lymphoid system. Front Immunol. 10:246. DOI: 10.3389/fimmu.2019.00246. PMID: 30886612. PMCID: PMC6410673.9. Ding Y, Zhou L, Xia Y, Wang W, Wang Y, Li L, et al. 2018; Reference values for peripheral blood lymphocyte subsets of healthy children in China. J Allergy Clin Immunol. 142:970–3. DOI: 10.1016/j.jaci.2018.04.022. PMID: 29746882.10. Warnatz K, Denz A, Dräger R, Braun M, Groth C, Wolff-Vorbeck G, et al. 2002; Severe deficiency of switched memory B cells (CD27(+)IgM(-)IgD(-)) in subgroups of patients with common variable immunodeficiency: a new approach to classify a heterogeneous disease. Blood. 99:1544–51. DOI: 10.1182/blood.V99.5.1544. PMID: 11861266.11. Del Pino-Molina L, López-Granados E, Lecrevisse Q, Torres Canizales J, Pérez-Andrés M, Blanco E, et al. 2021; Dissection of the pre-germinal center B-cell maturation pathway in common variable immunodeficiency based on standardized fFlow cytometric EuroFlow tools. Front Immunol. 11:603972. DOI: 10.3389/fimmu.2020.603972. PMID: 33679693. PMCID: PMC7925888.12. Delmonte OM, Schuetz C, Notarangelo LD. 2018; RAG deficiency: two genes, many Diseases. J Clin Immunol. 38:646–55. DOI: 10.1007/s10875-018-0537-4. PMID: 30046960. PMCID: PMC6643099.13. Kalina T, Bakardjieva M, Blom M, Perez-Andres M, Barendregt B, Kanderová V, et al. 2020; EuroFlow standardized approach to diagnostic immunopheneotyping of severe PID in newborns and young children. Front Immunol. 11:371. DOI: 10.3389/fimmu.2020.00371. PMID: 32265901. PMCID: PMC7096355.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection and Diagnosis of Primary Immunodeficiency Diseases
- Clinical Features of Primary Immunodeficiency Diseases
- A Case of Ankylosing Spondylitis in a Patient with Human Immunodeficiency Virus
- Genetic diagnosis of systemic autoinflammatory diseases and underlying primary immunodeficiency
- A Clinical Study of Primary Immunodeficiency Disease in a Single Center in Seoul from 1996 to 2004
