Clin Endosc.
2024 Jan;57(1):73-81. 10.5946/ce.2022.293.
Preclinical study of a novel ingestible bleeding sensor for upper gastrointestinal bleeding
- Affiliations
-
- 1Department of Medicine, Tufts University School of Medicine, Boston, MA, USA
- 2Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
- KMID: 2551195
- DOI: http://doi.org/10.5946/ce.2022.293
Abstract
- Background/Aims
Upper gastrointestinal bleeding (UGIB) is a life-threatening condition that necessitates early identification and intervention and is associated with substantial morbidity, mortality, and socioeconomic burden. However, several diagnostic challenges remain regarding risk stratification and the optimal timing of endoscopy. The PillSense System is a noninvasive device developed to detect blood in patients with UGIB in real time. This study aimed to assess the safety and performance characteristics of PillSense using a simulated bleeding model.
Methods
A preclinical study was performed using an in vivo porcine model (14 animals). Fourteen PillSense capsules were endoscopically placed in the stomach and blood was injected into the stomach to simulate bleeding. The safety and sensitivity of blood detection and pill excretion were also investigated.
Results
All the sensors successfully detected the presence or absence of blood. The minimum threshold was 9% blood concentration, with additional detection of increasing concentrations of up to 22.5% blood. All the sensors passed naturally through the gastrointestinal tract.
Conclusions
This study demonstrated the ability of the PillSense System sensor to detect UGIB across a wide range of blood concentrations. This ingestible device detects UGIB in real time and has the potential to be an effective tool to supplement the current standard of care. These favorable results will be further investigated in future clinical studies.
Keyword
Figure
-
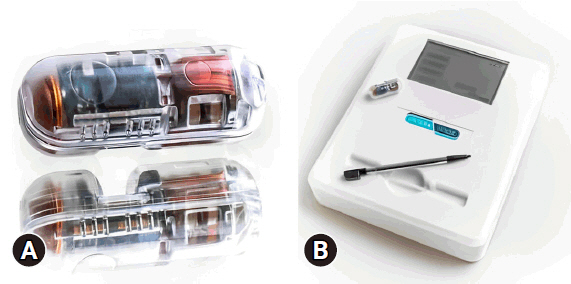
Fig. 1. PillSense System components. (A) PillSense capsule and (B) receiver. The PillSense System’s wireless communication system, consisting of internal optical sensors (A), links wirelessly to the external receiver and can relay data (B).

Fig. 2. Blood detection results in the acute study. The graph demonstrates increasing PillSense System sensor output as a function of increasing blood concentration in the stomach.
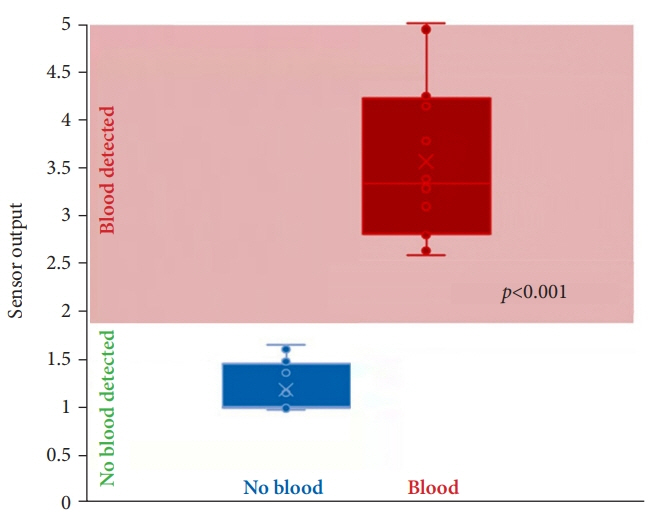
Fig. 3. Sensor output values recorded during survival study. All 12 sensors in the survival study detected a minimum blood concentration of 9%. There was a significant difference between the outputs of the sensor in the absence and presence of blood.

Reference
-
1. Wuerth BA, Rockey DC. Changing epidemiology of upper gastrointestinal hemorrhage in the last decade: a nationwide analysis. Dig Dis Sci. 2018; 63:1286–1293.2. Ghassemi KA, Jensen DM. Lower GI bleeding: epidemiology and management. Curr Gastroenterol Rep. 2013; 15:333.3. Lanas A, Perez-Aisa MA, Feu F, et al. A nationwide study of mortality associated with hospital admission due to severe gastrointestinal events and those associated with nonsteroidal antiinflammatory drug use. Am J Gastroenterol. 2005; 100:1685–1693.4. Tielleman T, Bujanda D, Cryer B. Epidemiology and risk factors for upper gastrointestinal bleeding. Gastrointest Endosc Clin N Am. 2015; 25:415–428.5. Antunes C, Copelin II EL. Upper gastrointestinal bleeding. StatPearls [Internet]. StatPearls Publishing;2022. [cited 2022 Aug 8]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK470300/.6. Wilkins T, Khan N, Nabh A, et al. Diagnosis and management of upper gastrointestinal bleeding. Am Fam Physician. 2012; 85:469–476.7. Kamboj AK, Hoversten P, Leggett CL. Upper gastrointestinal bleeding: etiologies and management. Mayo Clin Proc. 2019; 94:697–703.8. Abougergi MS, Travis AC, Saltzman JR. The in-hospital mortality rate for upper GI hemorrhage has decreased over 2 decades in the United States: a nationwide analysis. Gastrointest Endosc. 2015; 81:882–888.9. Jairath V, Kahan BC, Logan RF, et al. National audit of the use of surgery and radiological embolization after failed endoscopic haemostasis for non-variceal upper gastrointestinal bleeding. Br J Surg. 2012; 99:1672–1680.10. Balaban DV, Strâmbu V, Florea BG, et al. Predictors for in-hospital mortality and need for clinical intervention in upper GI bleeding: a 5-year observational study. Chirurgia (Bucur). 2014; 109:48–54.11. Aljarad Z, Mobayed BB. The mortality rate among patients with acute upper GI bleeding (with/without EGD) at Aleppo University Hospital: a retrospective study. Ann Med Surg (Lond). 2021; 71:102958.12. Jaka H, Koy M, Liwa A, et al. A fibreoptic endoscopic study of upper gastrointestinal bleeding at Bugando Medical Centre in northwestern Tanzania: a retrospective review of 240 cases. BMC Res Notes. 2012; 5:200.13. Hsu YC, Liou JM, Chung CS, et al. Early risk stratification with simple clinical parameters for cirrhotic patients with acute upper gastrointestinal bleeding. Am J Emerg Med. 2010; 28:884–890.14. Kumar AS, Sibia RS. Predictors of in-hospital mortality among patients presenting with variceal gastrointestinal bleeding. Saudi J Gastroenterol. 2015; 21:43–46.15. Katschinski B, Logan R, Davies J, et al. Prognostic factors in upper gastrointestinal bleeding. Dig Dis Sci. 1994; 39:706–712.16. Zimmerman J, Siguencia J, Tsvang E, et al. Predictors of mortality in patients admitted to hospital for acute upper gastrointestinal hemorrhage. Scand J Gastroenterol. 1995; 30:327–331.17. Javaid T, Siddiqui N, Hasan S, et al. The in-hospital mortality rate in gastrointestinal hemorrhage with shock: a nationwide analysis. Am Coll Gastroenterol. 2016; 111(Supplement 1):S420.18. Skok P, Sinkovič A. Upper gastrointestinal haemorrhage: predictive factors of in-hospital mortality in patients treated in the medical intensive care unit. J Int Med Res. 2011; 39:1016–1027.19. Gatta A, Merkel C, Amodio P, et al. Development and validation of a prognostic index predicting death after upper gastrointestinal bleeding in patients with liver cirrhosis: a multicenter study. Am J Gastroenterol. 1994; 89:1528–1536.20. Roberts SE, Button LA, Williams JG. Prognosis following upper gastrointestinal bleeding. PLoS One. 2012; 7:e49507.21. Garg SK, Anugwom C, Campbell J, et al. Early esophagogastroduodenoscopy is associated with better outcomes in upper gastrointestinal bleeding: a nationwide study. Endosc Int Open. 2017; 5:E376–E386.22. Barkun AN, Almadi M, Kuipers EJ, et al. Management of nonvariceal upper gastrointestinal bleeding: guideline recommendations from the International Consensus Group. Ann Intern Med. 2019; 171:805–822.23. Lau JY. Management of acute upper gastrointestinal bleeding: urgent versus early endoscopy. Dig Endosc. 2022; 34:260–264.24. Baxter A, Baxter A, Hearing S. PTU-39 Outcomes of urgent endoscopy delays during UK-wide lockdown at a teaching hospital. Gut. 2021; 70(Suppl 4):A61–A62.25. Jeong N, Kim KS, Jung YS, et al. Delayed endoscopy is associated with increased mortality in upper gastrointestinal hemorrhage. Am J Emerg Med. 2019; 37:277–280.26. Jacobs CC, Jaber JF, Ladna M, et al. Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission. Clin Gastroenterol Hepatol. 2021; 19:2648–2655.27. Laursen SB, Hansen JM, Schaffalitzky de Muckadell OB. The Glasgow Blatchford score is the most accurate assessment of patients with upper gastrointestinal hemorrhage. Clin Gastroenterol Hepatol. 2012; 10:1130–1135.28. Schembre DB, Ely RE, Connolly JM, et al. Semiautomated Glasgow-Blatchford bleeding score helps direct bed placement for patients with upper gastrointestinal bleeding. BMJ Open Gastroenterol. 2020; 7:e000479.29. Mustafa Z, Cameron A, Clark E, et al. Outpatient management of low-risk patients with upper gastrointestinal bleeding: can we safely extend the Glasgow Blatchford Score in clinical practice? Eur J Gastroenterol Hepatol. 2015; 27:512–515.30. Stephens JR, Hare NC, Warshow U, et al. Management of minor upper gastrointestinal haemorrhage in the community using the Glasgow Blatchford score. Eur J Gastroenterol Hepatol. 2009; 21:1340–1346.31. Srirajaskanthan R, Conn R, Bulwer C, et al. The Glasgow Blatchford scoring system enables accurate risk stratification of patients with upper gastrointestinal haemorrhage. Int J Clin Pract. 2010; 64:868–874.32. Laursen SB, Dalton HR, Murray IA, et al. Performance of new thresholds of the Glasgow Blatchford score in managing patients with upper gastrointestinal bleeding. Clin Gastroenterol Hepatol. 2015; 13:115–121.33. Masaoka T, Suzuki H, Hori S, et al. Blatchford scoring system is a useful scoring system for detecting patients with upper gastrointestinal bleeding who do not need endoscopic intervention. J Gastroenterol Hepatol. 2007; 22:1404–1408.34. Jung K, Moon W. Role of endoscopy in acute gastrointestinal bleeding in real clinical practice: an evidence-based review. World J Gastrointest Endosc. 2019; 11:68–83.35. Sittichanbuncha Y, Senasu S, Thongkrau T, et al. How to differentiate sites of gastrointestinal bleeding in patients with hematochezia by using clinical factors? Gastroenterol Res Pract. 2013; 2013:265076.36. Kovacs TO. Management of upper gastrointestinal bleeding. Curr Gastroenterol Rep. 2008; 10:535–542.37. DePriest J. Low incidence of hemodynamic instability in patients with gastrointestinal hemorrhage. South Med J. 1996; 89:386–390.38. Languasco A, Cazap N, Marciano S, et al. Hemoglobin concentration variations over time in general medical inpatients. J Hosp Med. 2010; 5:283–288.39. Cheung FK, Lau JY. Management of massive peptic ulcer bleeding. Gastroenterol Clin North Am. 2009; 38:231–243.40. Bhattarai M, Bansal P, Khan Y. Longest duration of retention of video capsule: a case report and literature review. World J Gastrointest Endosc. 2013; 5:352–355.41. Rondonotti E. Capsule retention: prevention, diagnosis and management. Ann Transl Med. 2017; 5:198.42. Kim BS, Li BT, Engel A, et al. Diagnosis of gastrointestinal bleeding: a practical guide for clinicians. World J Gastrointest Pathophysiol. 2014; 5:467–478.43. Meltzer AC, Pinchbeck C, Burnett S, et al. Emergency physicians accurately interpret video capsule endoscopy findings in suspected upper gastrointestinal hemorrhage: a video survey. Acad Emerg Med. 2013; 20:711–715.44. Brunk T, Schmidt A, Hochberger J, et al. Telemetric capsule-based upper gastrointestinal tract: blood detection: first multicentric experience. Minim Invasive Ther Allied Technol. 2022; 31:704–711.45. Chandran S, Testro A, Urquhart P, et al. Risk stratification of upper GI bleeding with an esophageal capsule. Gastrointest Endosc. 2013; 77:891–898.46. Sung JJ, Tang RS, Ching JY, et al. Use of capsule endoscopy in the emergency department as a triage of patients with GI bleeding. Gastrointest Endosc. 2016; 84:907–913.47. Marya NB, Jawaid S, Foley A, et al. A randomized controlled trial comparing efficacy of early video capsule endoscopy with standard of care in the approach to nonhematemesis GI bleeding (with videos). Gastrointest Endosc. 2019; 89:33–43.48. Gralnek IM, Ching JY, Maza I, et al. Capsule endoscopy in acute upper gastrointestinal hemorrhage: a prospective cohort study. Endoscopy. 2013; 45:12–19.49. Monteiro S, Gonçalves TC, Magalhães J, et al. Upper gastrointestinal bleeding risk scores: who, when and why? World J Gastrointest Pathophysiol. 2016; 7:86–96.50. Chatten K, Purssell H, Banerjee AK, et al. Glasgow Blatchford score and risk stratifications in acute upper gastrointestinal bleed: can we extend this to 2 for urgent outpatient management? Clin Med (Lond). 2018; 18:118–122.51. Banister T, Spiking J, Ayaru L. Discharge of patients with an acute upper gastrointestinal bleed from the emergency department using an extended Glasgow-Blatchford score. BMJ Open Gastroenterol. 2018; 5:e000225.52. Costa-Moreira P, Macedo G. Risk stratification in upper gastrointestinal bleeding: a measure of safety and efficiency in emergency care. GE Port J Gastroenterol. 2021; 28:231–233.53. Robertson M, Majumdar A, Boyapati R, et al. Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems. Gastrointest Endosc. 2016; 83:1151–1160.54. Kwack WG, Lim YJ. Current status and research into overcoming limitations of capsule endoscopy. Clin Endosc. 2016; 49:8–15.55. Gerson L, Lin OS. Cost-benefit analysis of capsule endoscopy compared with standard upper endoscopy for the detection of Barrett’s esophagus. Clin Gastroenterol Hepatol. 2007; 5:319–325.56. Van de Bruaene C, De Looze D, Hindryckx P. Small bowel capsule endoscopy: where are we after almost 15 years of use? World J Gastrointest Endosc. 2015; 7:13–36.57. Ziegler A, Gonzalez L, Blikslager A. Large animal models: the key to translational discovery in digestive disease research. Cell Mol Gastroenterol Hepatol. 2016; 2:716–724.58. Kararli TT. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm Drug Dispos. 1995; 16:351–380.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Could a bleeding-sensor device be established as a new paradigm for detecting upper gastrointestinal bleeding before performing endoscopy?
- Clinical Evaluation of Endoscopic Microwave Coagulation Therapy for Upper Gastrointestinal Bleeding
- Combined Upper Gastrointestinal Lesions with Esophageal Varices
- Recent Update of Embolization of Upper Gastrointestinal Tract Bleeding
- Endoscopic Management of Nonvariceal Upper Gastrointestinal Bleeding
