ERRATUM: Wire perforation of the missed tiny aneurysm originating from the fenestrated A1 segment during the endovascular approach
- Affiliations
-
- 1Department of Neurosurgery, Medical Research Institute, Pusan National University Hospital, School of Medicine Pusan National University, Busan, Korea
- KMID: 2549456
- DOI: http://doi.org/10.7461/jcen.2022.E2021.12.001.E
Figure
-

Fig. 1. Schematic diagram illustrating the strategy for clipping a small dorsal ICA aneurysm. A, B: Aneurysm was immediately exposed (A). Direct neck clipping was performed without removing the falciform ligament (B). C, D, E: Aneurysm was partially obscured by the falciform ligament (C). To expose it, the ligament was incised using a sickle knife (D). The aneurysm was sufficiently exposed to allow direct clipping without further partial ACP removal (E). F, G, H, I: Aneurysm was partially obscured by the falciform ligament (F). The aneurysm was not fully exposed after falciform ligament removal (G). After partial ACP removal, the fully exposed aneurysm (H) was clipped successfully (I). ICA, internal carotid artery; ACP, anterior clinoid process; FL, falciform ligament; ON, optic nerve
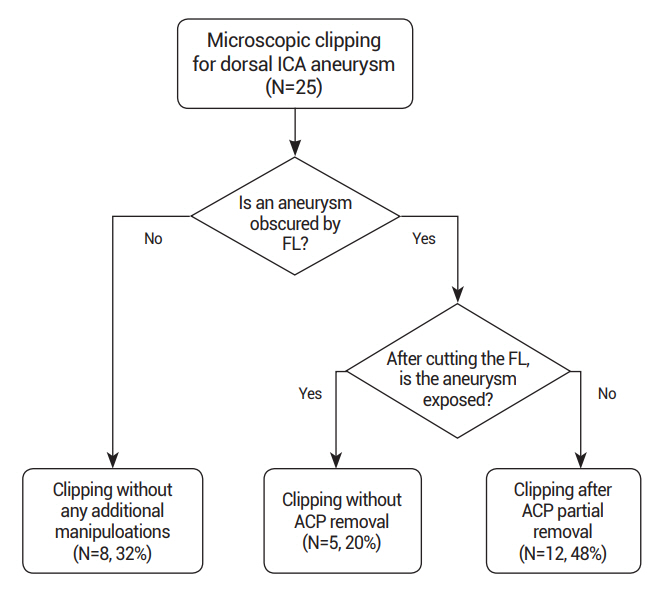
Fig. 2. Flow chart outlining the surgical strategies. ICA, internal carotid artery; FL, falciform ligament; ACP, anterior clinoid process
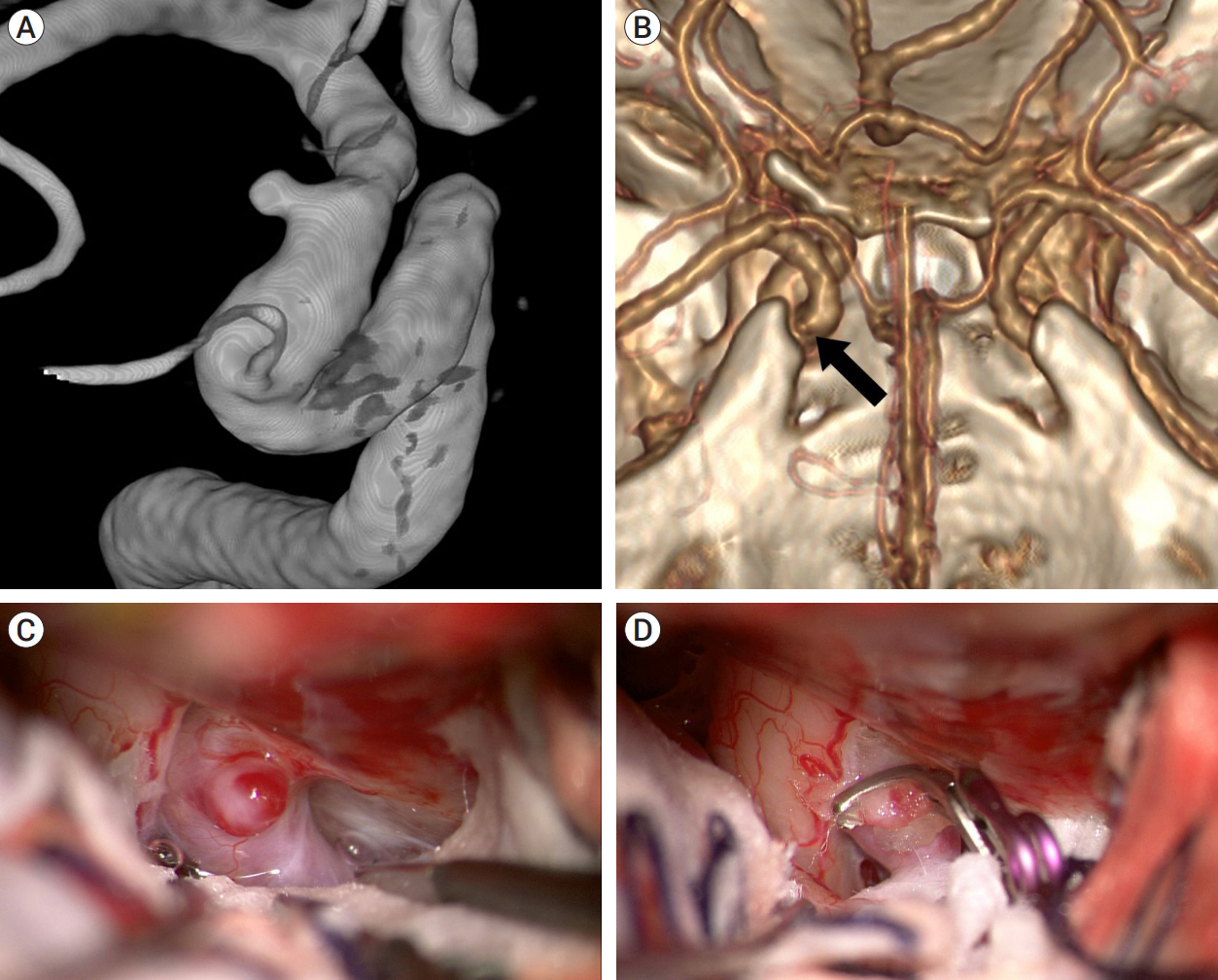
Fig. 3. Case illustration 1: Aneurysm clipped without the need to cut the falciform ligament. (A) On the 25° rotated digital subtraction angiography image, a dorsal ICA aneurysm is observed distal to the ophthalmic artery. (B) 3D CTA with bone image revealed that the aneurysm (arrow) was situated distally to the ACP. (C) The aneurysm was not obscured by the falciform ligament. (D) The aneurysm was clipped without cutting the falciform ligament. ICA, internal carotid artery; CTA, computed tomography angiography; ACP, anterior clinoid process
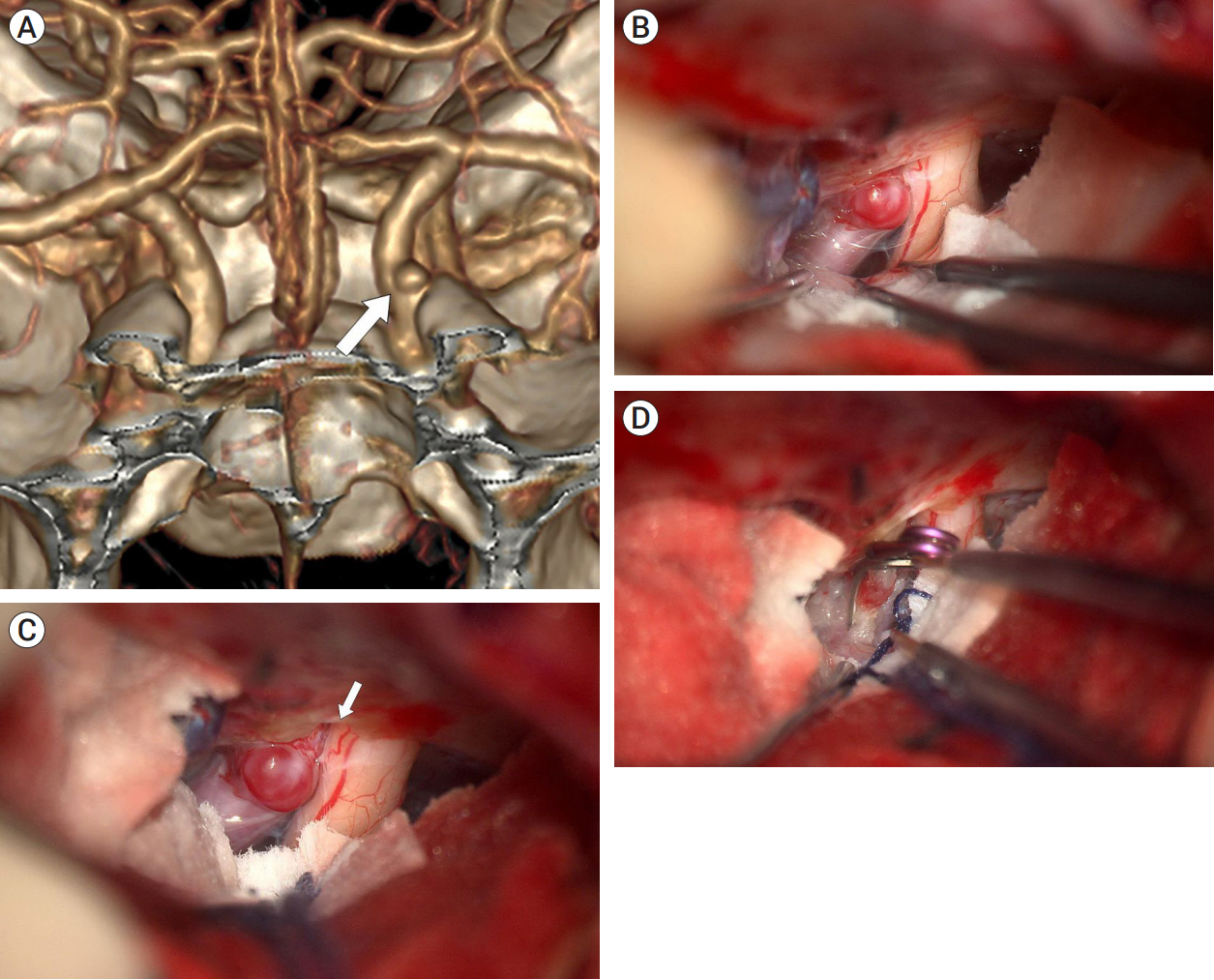
Fig. 4. Case illustration 2: Aneurysm clipped with only the falciform ligament being cut. (A) 3D CTA with bone image revealed that aneurysm (white arrow) was located distal to ACP. (B) The aneurysm obscured by the falciform ligament. (C) Aneurysm after cutting of the falciform ligament (white arrow). (D) The aneurysm was fully exposed, allowing for successful clipping without the ACP removal. CTA, computed tomography angiography; ACP, anterior clinoid process
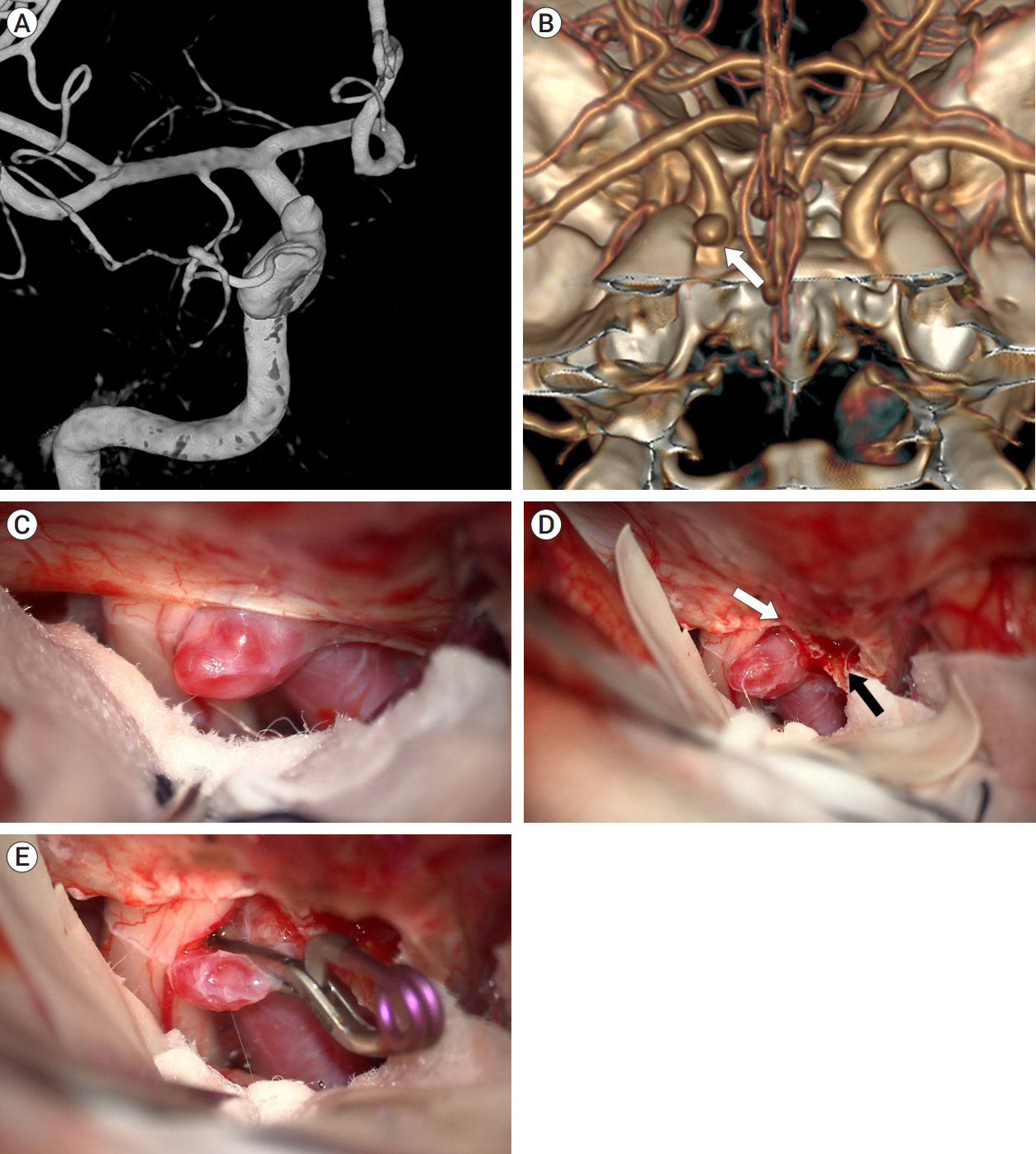
Fig. 5. Case illustration 3: Aneurysm clipped with both the falciform ligament being cut and partial removal of the ACP. (A) Preoperative digital subtraction angiography revealed an aneurysm with a bleb situated distal to the ophthalmic artery. (B) 3D CTA with bone image showed that the aneurysm (white arrow) was located medial to the ACP, rather than distal to it. (C) The aneurysm was obscured by the falciform ligament. (D) After cutting of the falciform ligament (white arrow), partial removal of the ACP (black arrow) was performed for improved exposure of the aneurysm. (E) The aneurysm was successfully clipped. ACP, anterior clinoid process; CTA, computed tomography angiography
Reference
-
1. Geyik S, Yavuz K, Yurttutan N, Saatci I, Cekirge HS. Stent-assisted coiling in endovascular treatment of 500 consecutive cerebral aneurysms with long-term follow-up. AJNR Am J Neuroradiol. 2013; Nov-Dec. 34(11):2157–62.2. Hong CK, Ahn JY, Joo JY. Internal carotid artery trunk aneurysms-management and outcome. Korean Journal of Cerebrovascular Surgery. 2006; 8(2):91–5.3. Kachhara R, Nair S, Nigam P. Ophthalmic segment aneurysms: Surgical treatment and outcomes. J Neurosci Rural Pract. 2021; Oct. 12(4):635–41.4. Koivisto T, Vanninen R, Hurskainen H, Saari T, Hernesniemi J, Vapalahti M. Outcomes of early endovascular versus surgical treatment of ruptured cerebral aneurysms. A prospective randomized study. Stroke. 2000; Oct. 31(10):2369–77.5. Krisht AF, Hsu SP. Paraclinoid aneurysms: Part 1: Superior (true ophthalmic) aneurysms. Contemporary Neurosurgery. 2008; 30(15):1–5.6. Kulwin C, Tubbs RS, Cohen-Gadol AA. Anterior clinoidectomy: Description of an alternative hybrid method and a review of the current techniques with an emphasis on complication avoidance. Surg Neurol Int. 2011; 2:140.7. Kwon BJ, Im SH, Park JC, Cho YD, Kang HS, Kim JE, et al. Shaping and navigating methods of microcatheters for endovascular treatment of paraclinoid aneurysms. Neurosurgery. 2010; Jul. 67(1):34–40. discussion 40.8. Larson JJ, Tew JM Jr, Tomsick TA, van Loveren HR. Treatment of aneurysms of the internal carotid artery by intravascular balloon occlusion: Long-term follow-up of 58 patients. Neurosurgery. 1995; Jan. 36(1):26–30. discussion 30.9. Liu J, Jing L, Wang C, Paliwal N, Wang S, Zhang Y, et al. Effect of hemodynamics on outcome of subtotally occluded paraclinoid aneurysms after stent-assisted coil embolization. J Neurointerv Surg. 2016; Nov. 8(11):1140–7.10. McDougall CG, Spetzler RF, Zabramski JM, Partovi S, Hills NK, Nakaji P, et al. The barrow ruptured aneurysm trial. J Neurosurg. 2012; Jan. 116(1):135–44.11. Mitchell PJ, Muthusamy S, Dowling R, Yan B. Does small aneurysm size predict intraoperative rupture during coiling in ruptured and unruptured aneurysms? J Stroke Cerebrovasc Dis. 2013; Nov. 22(8):1298–303.12. Molyneux A, Kerr R; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group, Stratton I, Sandercock P, Clarke M, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomized trial. J Stroke Cerebrovasc Dis. 2002; Nov-Dec. 11(6):304–14.13. Ries T, Buhk JH, Kucinski T, Goebell E, Grzyska U, Zeumer H, et al. Intravenous administration of acetylsalicylic acid during endovascular treatment of cerebral aneurysms reduces the rate of thromboembolic events. Stroke. 2006; Jul. 37(7):1816–21.14. Ryttlefors M, Enblad P, Kerr RS, Molyneux AJ. International subarachnoid aneurysm trial of neurosurgical clipping versus endovascular coiling: Subgroup analysis of 278 elderly patients. Stroke. 2008; Oct. 39(10):2720–6.15. Shin DS, Carroll CP, Elghareeb M, Hoh BL, Kim BT. The evolution of flow-diverting stents for cerebral aneurysms; Historical review, modern application, complications, and future direction. J Korean Neurosurg Soc. 2020; Mar. 63(2):137–52.16. Song J, Kim BS, Shin YS. Treatment outcomes of unruptured intracranial aneurysm; Experience of 1,231 consecutive aneurysms. Acta Neurochir (Wien). 2015; Sep. 157(8):1303–10. discussion 1311.17. Szmuda T, Sloniewski P, Ali S, Kamieniecki A, Dzierzanowski J. Extent of anterior clinoidectomy for clipping of carotid-ophthalmic aneurysms predicted on three-dimensional computerised tomography angiography. Neurol Neurochir Pol. 2020; 54(2):138–49.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wire perforation of the missed tiny aneurysm originating from the fenestrated A1 segment during the endovascular approach
- Ruptured Saccular Aneurysm Arising from Fenestrated Proximal Anterior Cerebral Artery : Case Report and Literature Review
- Fusiform Aneurysm of Proximal Anterior Cerebral Artery: Case Report
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Fenestrated Endovascular Aneurysm Repair versus Snorkel Endovascular Aneurysm Repair: Competing yet Complementary Strategies
