Unusual presentation of asymptomatic subacute lead-related ventricular perforation beyond the pericardium without pericardial effusion: a case report
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Jeonbuk National University Hospital and Jeonbuk National University Medical School, Jeonju, Korea
- 2Research Institute of Clinical Medicine, Jeonbuk National University, Jeonju, Korea
- 3Biomedical Research Institute, Jeonbuk National University Hospital, Jeonju, Korea
- KMID: 2548350
- DOI: http://doi.org/10.12701/jyms.2023.00171
Abstract
- The clinical manifestations of subacute pacemaker lead-related cardiac perforations are highly variable. Patients with subacute perforations can present with a variety of symptoms, whereas those with acute perforations usually present with cardiac tamponade that necessitates emergent pericardiocentesis. A 32-year-old woman underwent pacemaker implantation for sick sinus syndrome. An active-fixation atrial lead was fixed to the right atrial appendage, and a ventricular lead was fixed to the right ventricle (RV) apex, with acceptable parameters. Two weeks postoperative, the patient visited the clinic for routine examination of the pacemaker parameters. Chest X-ray showed migration of the RV lead beyond the cardiac silhouette. Echocardiography revealed no evidence of pericardial effusion or tamponade. Computed tomography revealed that the RV lead was positioned beyond the RV and pericardium and into the anterior chest wall. Procedural lead revision was performed with cardiothoracic surgery backup. The lead was retracted after loosening the active-fixation screw and inserting the stylet. The lead was placed in the RV septum with active fixation. The procedure was completed without complications, and the patient was discharged after 3 days. Subacute lead perforations can present with various symptoms, and some patients may be asymptomatic without pericardial effusion. Altered lead parameters frequently provide the first indication for the diagnosis of cardiac perforation. Transvenous lead revision with surgical backup is an alternative to surgical extraction.
Figure
-
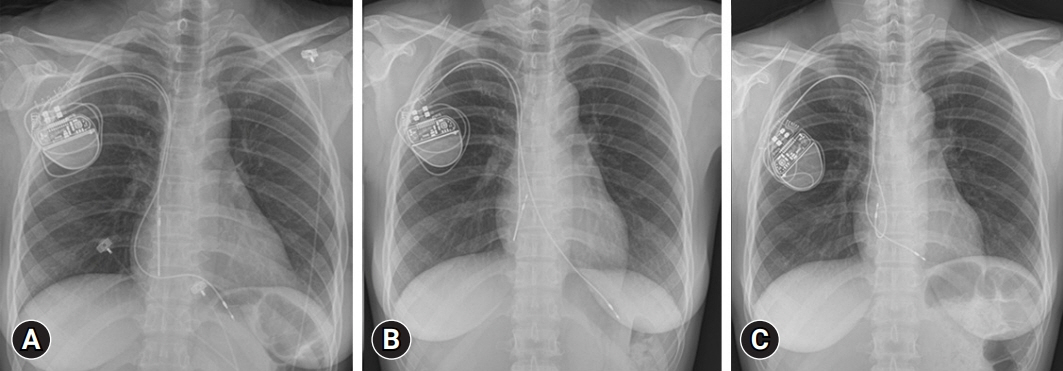
Fig. 1. Chest X-ray findings. (A) The next day after the first procedure. The ventricular lead is positioned near the right ventricle (RV) apex. (B) Two weeks later a routine check-up. The ventricular lead tip is located beyond the cardiac silhouette, which suggests a lead-related cardiac perforation. (C) After pacemaker lead revision. Transvenous procedural lead revision allows the lead to enter the RV cavity, reposition near the RV mid-septum, and fix in place.
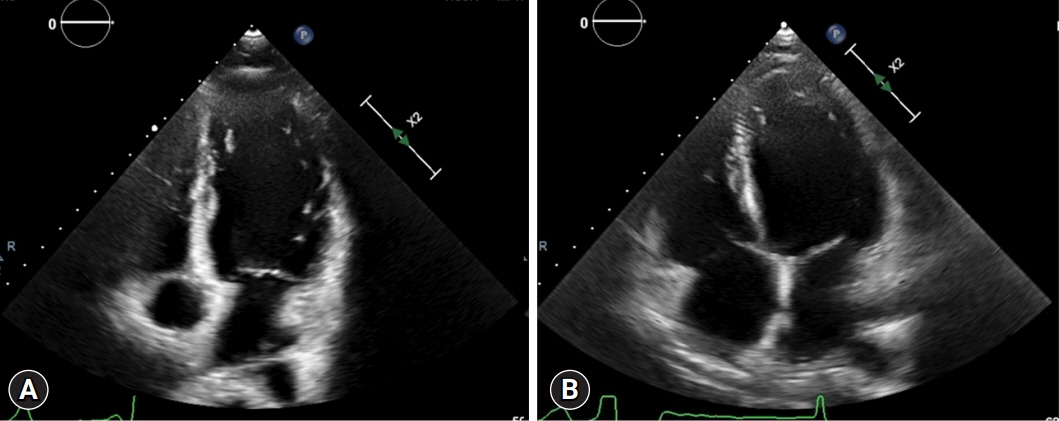
Fig. 2. (A) Echocardiographic finding prior to pacemaker implantation. (B) Echocardiographic finding after lead-related cardiac perforation. There is no evidence of pericardial effusion or tamponade on the apical four-chamber view.
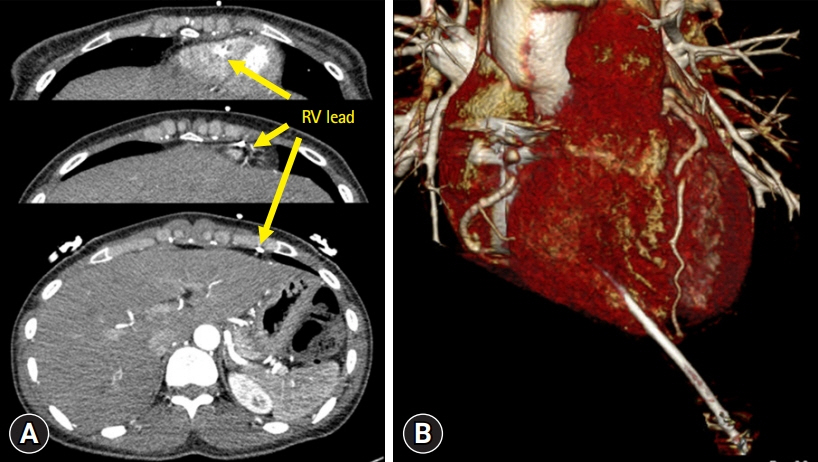
Fig. 3. Chest computed tomography (CT) findings. (A) Axial CT images show that the right ventricle (RV) lead (arrows) is positioned beyond the RV and pericardium and into the anterior chest wall. (B) Three-dimensional CT image clearly shows that the RV lead has pierced the cardiac wall.
Reference
-
References
1. Vamos M, Erath JW, Benz AP, Bari Z, Duray GZ, Hohnloser SH. Incidence of cardiac perforation with conventional and with leadless pacemaker systems: a systematic review and meta-analysis. J Cardiovasc Electrophysiol. 2017; 28:336–46.
Article2. Issa ZF, Issa TZ. Feasibility and safety of percutaneous lead revision for subacute and delayed cardiac device lead perforation. JACC Clin Electrophysiol. 2021; 7:26–35.
Article3. Archontakis S, Sideris K, Aggeli K, Gatzoulis K, Demosthenous M, Tolios P, et al. Percutaneous lead extraction and repositioning: an effective and safe therapeutic strategy for early ventricular lead perforation with dislocation both inside and outside the pericardial sac following a cardiac device implantation. J Cardiovasc Electrophysiol. 2019; 30:299–307.
Article4. Zhou X, Ze F, Li D, Wang L, Guo J, Li X. Outcomes of transvenous lead extraction in patients with lead perforation: a single-center experience. Clin Cardiol. 2020; 43:386–93.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Medistinal Teratoma with Pleural and Pericardial Effusion Teratoma with Pleural and Pericardial Effusion
- Right Ventricular Perforation and Left Hemothorax by Permanent Transveneous Pacemaker Lead: Report of 1 Case
- Delayed Perforation of the Right Ventricular Wall by a Single Standard-Caliber Implantable Cardioverter-Defibrillator Lead Detected by Multidetector Computed Tomography
- CT Findings of Tuberculous Pericardial Effusion
- Primary Intrapericardial Lipoma Simulating Pericardial Effusion -Report of A Case-
