J Korean Neurosurg Soc.
2023 Nov;66(6):690-702. 10.3340/jkns.2023.0033.
Clinical Outcomes of Coil Embolization for Unruptured Intracranial Aneurysms Categorized by Region and Hospital Size : A Nationwide Cohort Study in Korea
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 2Department of Neurosurgery, Chungnam National University Sejong Hospital, Chungnam National University College of Medicine, Daejoen, Korea
- KMID: 2547463
- DOI: http://doi.org/10.3340/jkns.2023.0033
Abstract
Objective
: To analyze the outcomes of coil embolization (CE) for unruptured intracranial aneurysm (UIA) according to region and hospital size based on National Health Insurance Service data in South Korea.
Methods
: The incidence of complications, including intracranial hemorrhage (ICRH) and cerebral infarction (CI), occurring within 3 months and the 1-year mortality rates in UIA patients who underwent CE in 2018 were analyzed. Hospitals were classified as tertiary referral general hospitals (TRGHs), general hospitals (GHs) or semigeneral hospitals (sGHs) according to their size, and the administrative districts of South Korea were divided into 15 regions.
Results
: In 2018, 8425 (TRGHs, 4438; GHs, 3617; sGHs, 370) CEs were performed for UIAs. Complications occurred in 5.69% of patients seen at TRGHs, 13.48% at GHs, and 20.45% at sGHs. The complication rate in TRGHs was significantly lower than that in GHs (p=0.039) or sGHs (p=0.005), and that in GHs was significantly lower than that in sGHs (p=0.030). The mortality rates in TRGHs, GHs, and sGHs were 0.81%, 2.16%, and 3.92%, respectively, with no significant difference. Despite no significant difference in the mortality rates, the complication rate significantly increased as the number of CE procedures per hospital decreased (p=0.001; rho=-0.635). Among the hospitals where more than 30 CEs were performed for UIAs, the incidence of CIs (p=0.096, rho=-0.205) and the mortality rates (3 months, p=0.048, rho=-0.243; 1 year, p=0.009, rho=-0.315) significantly decreased as the number of CEs that were performed increased and no significant difference in the incidence of post-CE ICRH was observed.
Conclusion
: The complication rate in patients who underwent CE for UIA increased as the hospital size and physicians’ experience in conducting CEs decreased. We recommend nationwide quality control policies CEs for UIAs.
Figure
-
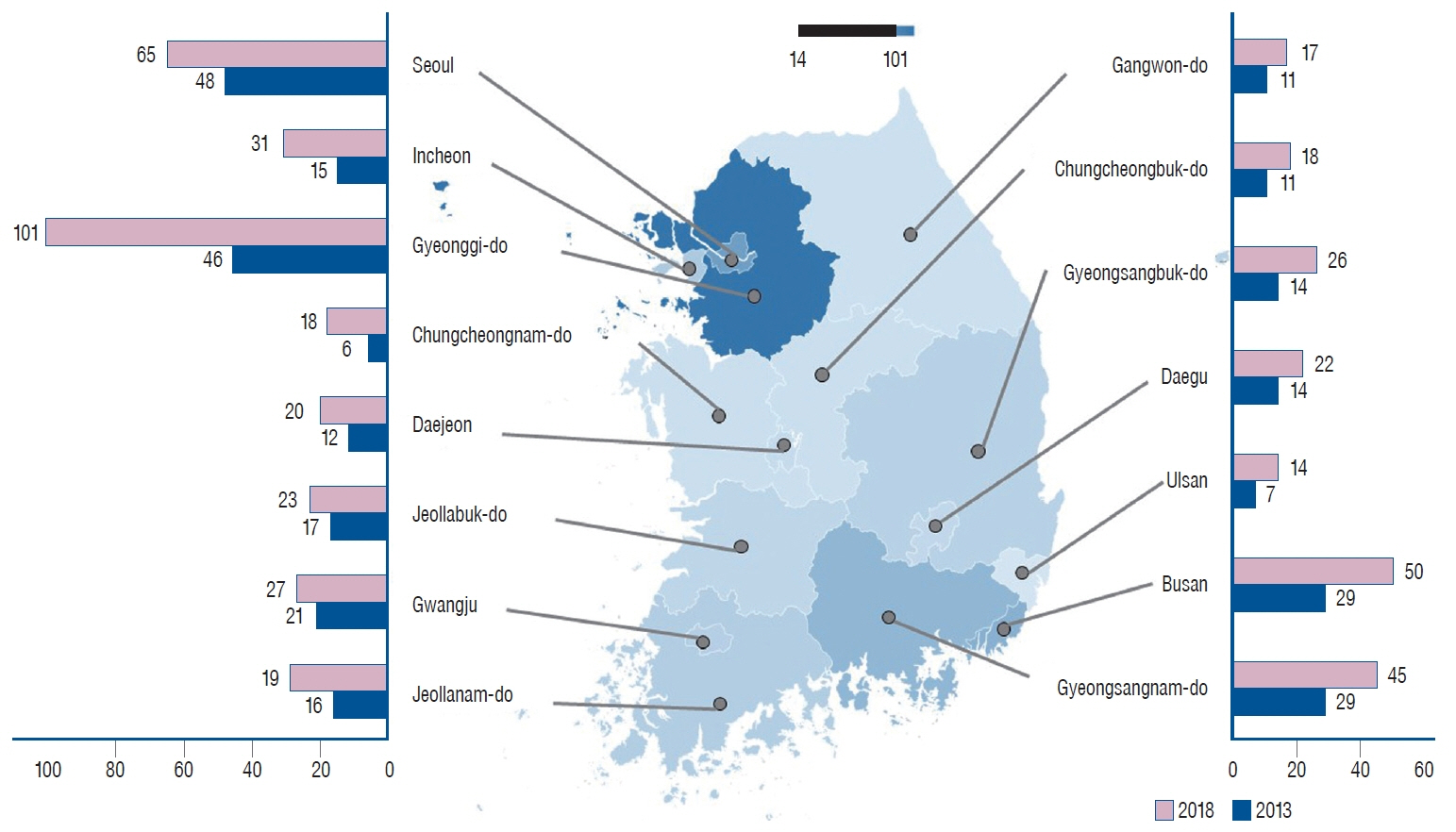
Fig. 1. Number of hospitals performing coil embolization for unruptured intracranial aneurysms, categorized by region and hospital size.
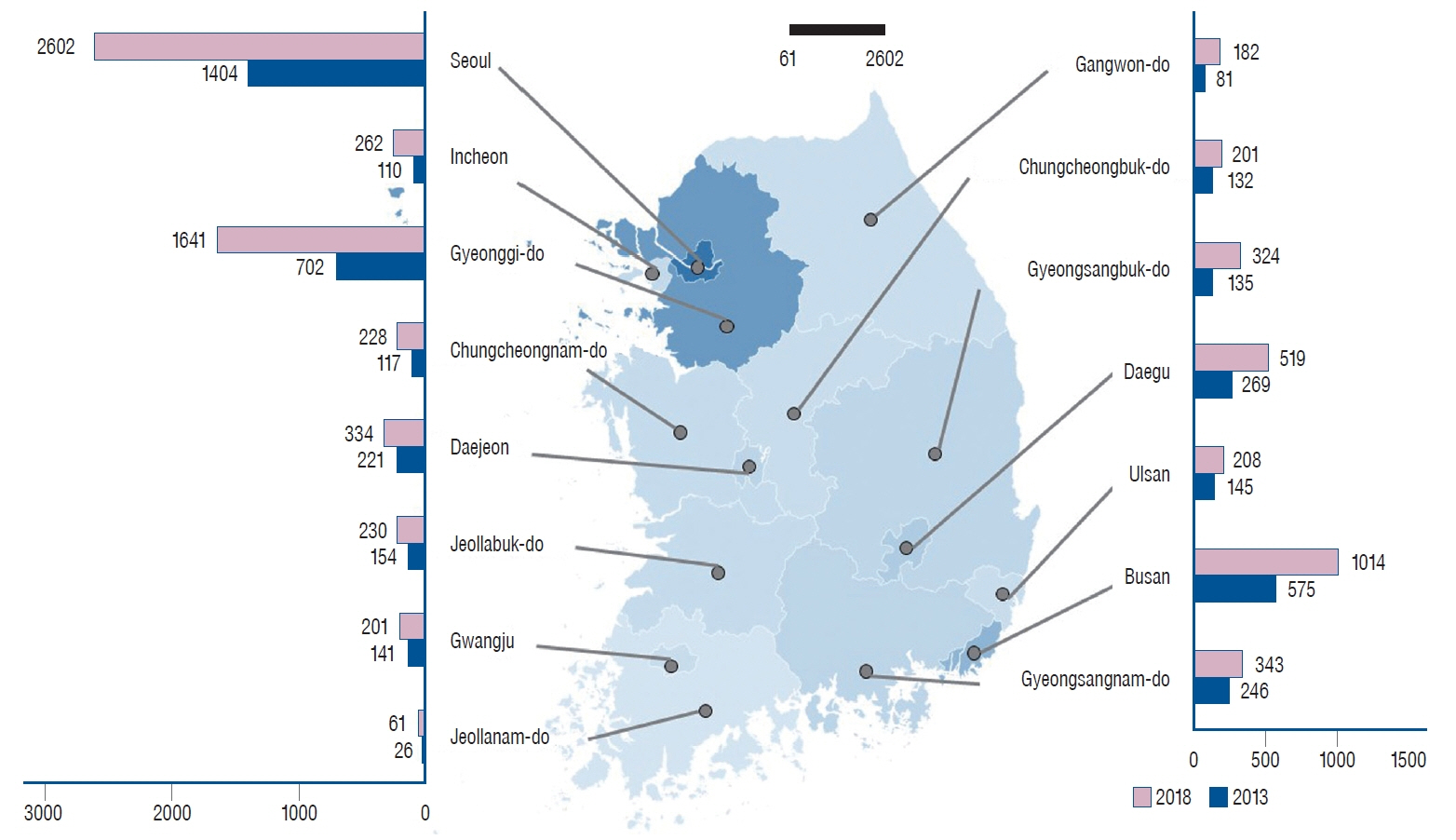
Fig. 2. Number of coil embolization procedures for unruptured intracranial aneurysms, categorized by region and hospital size.
Reference
-
References
1. Chalouhi N, Jabbour P, Singhal S, Drueding R, Starke RM, Dalyai RT, et al. Stent-assisted coiling of intracranial aneurysms: predictors of complications, recanalization, and outcome in 508 cases. Stroke. 44:1348–1353. 2013.2. Chien SC, Chen CC, Chen CT, Wang AY, Hsieh PC, Yeap MC, et al. Ticagrelor versus clopidogrel in stent-assisted coil embolization of unruptured intracranial aneurysms. Interv Neuroradiol. 28:568–574. 2022.
Article3. Choi HH, Cho YD, Yoo DH, Ahn SJ, Cho WS, Kang HS, et al. Stentassisted coil embolization of anterior communicating artery aneurysms: safety, effectiveness, and risk factors for procedural complications or recanalization. J Neurointerv Surg. 11:49–56. 2019.
Article4. Feng MT, Wen WL, Feng ZZ, Fang YB, Liu JM, Huang QH. Endovascular embolization of intracranial aneurysms: to use stent(s) or not? systematic review and meta-analysis. World Neurosurg. 93:271–278. 2016.
Article5. Gonda DD, Khalessi AA, McCutcheon BA, Marcus LP, Noorbakhsh A, Chen CC, et al. Long-term follow-up of unruptured intracranial aneurysms repaired in California. J Neurosurg. 120:1349–1357. 2014.
Article6. Higashi E, Matsumoto S, Nakahara I, Hatano T, Ishii A, Sadamasa N, et al. Clopidogrel response predicts thromboembolic events associated with coil embolization of unruptured intracranial aneurysms: a prospective cohort study. PLoS One. 16:e0249766. 2021.
Article7. Hoh BL, Rabinov JD, Pryor JC, Carter BS, Barker FG 2nd. In-hospital morbidity and mortality after endovascular treatment of unruptured intracranial aneurysms in the United States, 1996-2000: effect of hospital and physician volume. AJNR Am J Neuroradiol. 24:1409–1420. 2003.8. Hwang G, Huh W, Lee JS, Villavicencio JB, Villamor RB Jr, Ahn SY, et al. Standard vs modified antiplatelet preparation for preventing thromboembolic events in patients with high on-treatment platelet reactivity undergoing coil embolization for an unruptured intracranial aneurysm: a randomized clinical trial. JAMA Neurol. 72:764–772. 2015.
Article9. Im SH, Han MH, Kwon OK, Kwon BJ, Kim SH, Kim JE, et al. Endovascular coil embolization of 435 small asymptomatic unruptured intracranial aneurysms: procedural morbidity and patient outcome. AJNR Am J Neuroradiol. 30:79–84. 2009.
Article10. Kabbasch C, Goertz L, Siebert E, Herzberg M, Borggrefe J, Mpotsaris A, et al. Comparison of WEB embolization and coiling in unruptured intracranial aneurysms: safety and efficacy based on a propensity score analysis. World Neurosurg. 126:e937–e943. 2019.
Article11. Kim B, Kim K, Jeon P, Kim S, Kim H, Byun H, et al. Thromboembolic complications in patients with clopidogrel resistance after coil embolization for unruptured intracranial aneurysms. AJNR Am J Neuroradiol. 35:1786–1792. 2014.
Article12. Kim T, Lee H, Ahn S, Kwon OK, Bang JS, Hwang G, et al. Incidence and risk factors of intracranial aneurysm: a national cohort study in Korea. Int J Stroke. 11:917–927. 2016.
Article13. Kim YD, Kwon OK, Ban SP, Won YD, Bang JS, Kim T, et al. The inhibition rate estimated using VerifyNow can help to predict the thromboembolic risk of coil embolization for unruptured intracranial aneurysms. J Neurointerv Surg. 14:589–592. 2022.
Article14. Lee SH, Lee SU, Kwon OK, Bang JS, Ban SP, Kim T, et al. Clinical outcomes of clipping and coiling in elderly patients with unruptured cerebral aneurysms: a national cohort study in Korea. J Korean Med Sci. 36:e178. 2021.
Article15. Lee SU, Kim T, Kwon OK, Bang JS, Ban SP, Byoun HS, et al. Trends in the incidence and treatment of cerebrovascular diseases in Korea : part I. Intracranial aneurysm, intracerebral hemorrhage, and arteriovenous malformation. J Korean Neurosurg Soc. 63:56–68. 2020.
Article16. Lee SU, Kim T, Kwon OK, Bang JS, Ban SP, Byoun HS, et al. Trends in the incidence and treatment of cerebrovascular diseases in Korea : part II. Cerebral infarction, cerebral arterial stenosis, and moyamoya disease. J Korean Neurosurg Soc. 63:69–79. 2020.
Article17. Leifer D, Fonarow GC, Hellkamp A, Baker D, Hoh BL, Prabhakaran S, et al. Association between hospital volumes and clinical outcomes for patients with nontraumatic subarachnoid hemorrhage. J Am Heart Assoc. 10:e018373. 2021.
Article18. Lin N, Cahill KS, Frerichs KU, Friedlander RM, Claus EB. Treatment of ruptured and unruptured cerebral aneurysms in the USA: a paradigm shift. J Neurointerv Surg. 4:182–189. 2012.
Article19. Lindgren A, Burt S, Bragan Turner E, Meretoja A, Lee JM, Hemmen TM, et al. Hospital case-volume is associated with case-fatality after aneurysmal subarachnoid hemorrhage. Int J Stroke. 14:282–289. 2019.
Article20. Luther E, McCarthy DJ, Brunet MC, Sur S, Chen SH, Sheinberg D, et al. Treatment and diagnosis of cerebral aneurysms in the post-international subarachnoid aneurysm trial (ISAT) era: trends and outcomes. J Neurointerv Surg. 12:682–687. 2020.
Article21. Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the international subarachnoid aneurysm trial (ISAT). Lancet. 385:691–697. 2015.
Article22. Molyneux AJ, Kerr RS, Birks J, Ramzi N, Yarnold J, Sneade M, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): longterm follow-up. Lancet Neurol. 8:427–433. 2009.
Article23. Nii K, Inoue R, Morinaga Y, Mitsutake T, Hanada H. Evaluation of acute in-stent thrombosis during stent-assisted coil embolization of unruptured intracranial aneurysms. Neurol Med Chir (Tokyo). 58:435–441. 2018.
Article24. Nishido H, Piotin M, Bartolini B, Pistocchi S, Redjem H, Blanc R. Analysis of complications and recurrences of aneurysm coiling with special emphasis on the stent-assisted technique. AJNR Am J Neuroradiol. 35:339–344. 2014.
Article25. Pierot L, Spelle L, Vitry F; ATENA Investigators. Immediate clinical outcome of patients harboring unruptured intracranial aneurysms treated by endovascular approach: results of the ATENA study. Stroke. 39:2497–2504. 2008.
Article26. Sedat J, Chau Y, Gaudart J, Sachet M, Beuil S, Lonjon M. Prasugrel versus clopidogrel in stent-assisted coil embolization of unruptured intracranial aneurysms. Interv Neuroradiol. 23:52–59. 2017.
Article27. Standhardt H, Boecher-Schwarz H, Gruber A, Benesch T, Knosp E, Bavinzski G. Endovascular treatment of unruptured intracranial aneurysms with Guglielmi detachable coils: short- and long-term results of a single-centre series. Stroke. 39:899–904. 2008.
Article28. Tykocki T, Kostyra K, Czyż M, Kostkiewicz B. Four-year trends in the treatment of cerebral aneurysms in Poland in 2009-2012. Acta Neurochir (Wien). 156:861–868. 2014.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Complications after Uneventful Coil Embolization of Unruptured Aneurysms : Case Report
- Unruptured Aneurysms-Endovascular Treatment
- Clinical Experience of Thromboembolic Complications of Coil Embolization for Intracranial Aneurysms with Literature Review
- Self-Efficacy and Self-Care Behavior in Patients with Unruptured Intracranial Aneurysm after Treatment with Coil Embolization
- Ruptured Very Small Cerebral Aneurysms and the Usefulness of Coil Embolization
