Interleukin-6-producing paraganglioma as a rare cause of systemic inflammatory response syndrome: a case report
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Daegu Veterans Hospital, Daegu, Korea
- 2Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea
- KMID: 2547370
- DOI: http://doi.org/10.12701/jyms.2022.00766
Abstract
- Pheochromocytomas and paragangliomas (PPGLs) may secrete hormones or bioactive neuropeptides such as interleukin-6 (IL-6), which can mask the clinical manifestations of catecholamine hypersecretion. We report the case of a patient with delayed diagnosis of paraganglioma due to the development of IL-6-mediated systemic inflammatory response syndrome (SIRS). A 58-year-old woman presented with dyspnea and flank pain accompanied by SIRS and acute cardiac, kidney, and liver injuries. A left paravertebral mass was incidentally observed on abdominal computed tomography (CT). Biochemical tests revealed increased 24-hour urinary metanephrine (2.12 mg/day), plasma norepinephrine (1,588 pg/mL), plasma normetanephrine (2.27 nmol/L), and IL-6 (16.5 pg/mL) levels. 18F-fluorodeoxyglucose (FDG) positron emission tomography/CT showed increased uptake of FDG in the left paravertebral mass without metastases. The patient was finally diagnosed with functional paraganglioma crisis. The precipitating factor was unclear, but phendimetrazine tartrate, a norepinephrine-dopamine release drug that the patient regularly took, might have stimulated the paraganglioma. The patient’s body temperature and blood pressure were well controlled after alpha-blocker administration, and the retroperitoneal mass was surgically resected successfully. After surgery, the patient’s inflammatory, cardiac, renal, and hepatic biomarkers and catecholamine levels improved. In conclusion, our report emphasizes the importance of IL-6-producing PPGLs in the differential diagnosis of SIRS.
Keyword
Figure
-
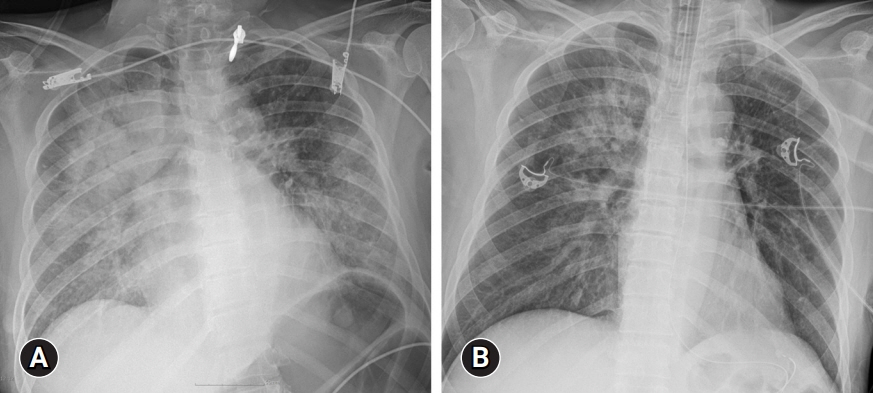
Fig. 1. (A) Chest X-ray performed at admission shows bilateral lung infiltrations. (B) Follow-up chest X-ray performed 24-hour after admission shows prominent resolution of the lung infiltrations.
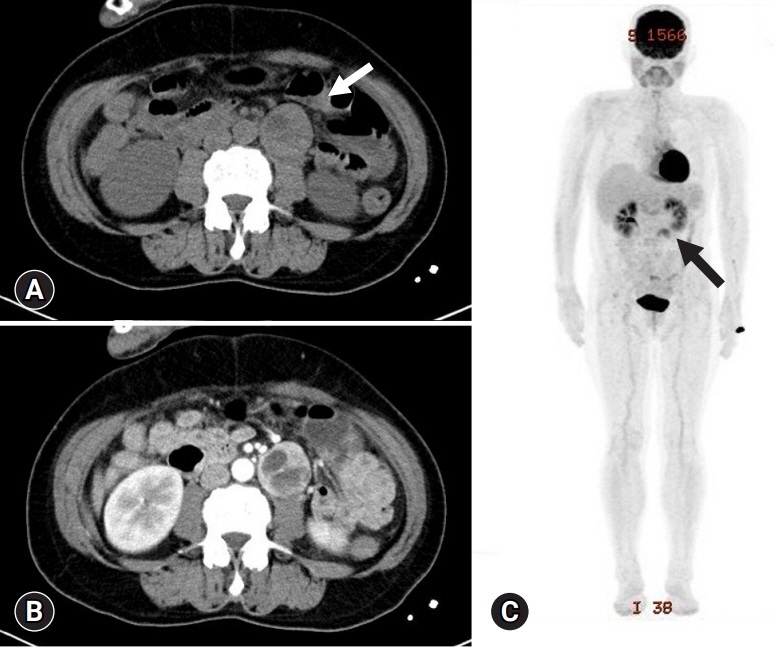
Fig. 2. (A) Abdominal CT scan demonstrates the presence of a 3.8 cm-long round mass originating from the left paravertebral area. Non-enhanced attenuation of the mass reaches more than 20 Hounsfield units (arrow). (B) In the arterial phase, the tumor is heterogeneously enhanced with partial cystic changes. (C) 18F-fluorodeoxyglucose PET-CT scan demonstrates increased uptake (arrow) in the mass originating in the left paravertebral area and no metastases. CT, computed tomography; PET, positron emission tomography.
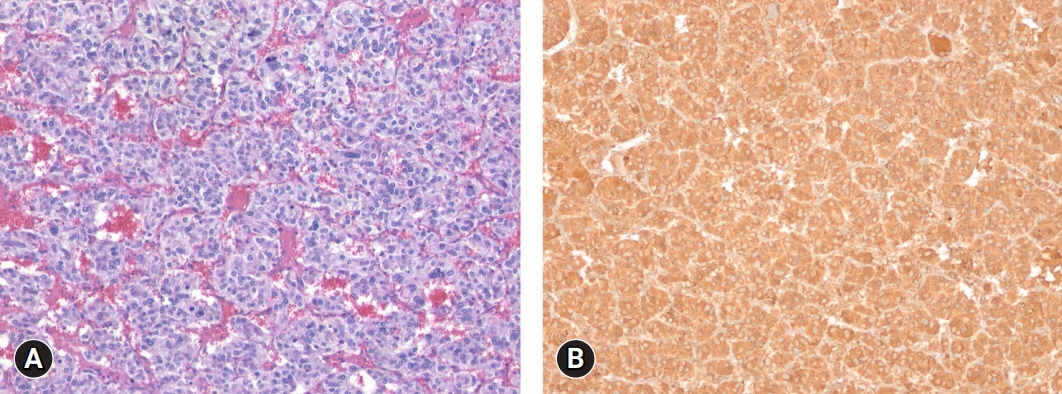
Fig. 3. Histologic and Immunohistochemical findings. (A) The tumor cells have abundant basophilic cytoplasm. A prominent cell-nesting pattern (zellballen) is noted (hematoxylin and eosin stain, ×100). (B) Tumor cells are diffusely positive for chromogranin A (immunohistochemical stain, ×100).
Reference
-
References
1. Whitelaw BC, Prague JK, Mustafa OG, Schulte KM, Hopkins PA, Gilbert JA, et al. Phaeochromocytoma [corrected] crisis. Clin Endocrinol (Oxf). 2014; 80:13–22.2. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014; 6:a016295.
Article3. Akira S, Hirano T, Taga T, Kishimoto T. Biology of multifunctional cytokines: IL 6 and related molecules (IL 1 and TNF). FASEB J. 1990; 4:2860–7.
Article4. Carvalho Cunha N, Gomes L, Saraiva J, Paiva I. Interleukin-6 producing pheochromocytoma: a rare cause of systemic inflammatory response syndrome. Case Rep Endocrinol. 2019; 2019:7906272.
Article5. Meijs AC, Schroijen MA, Snel M, Corssmit EP. Interleukin-6 producing pheochromocytoma/paraganglioma: case series from a tertiary referral centre for pheochromocytomas and paragangliomas. J Endocrinol Invest. 2021; 44:2253–9.
Article6. Angelousi A, Peppa M, Chrisoulidou A, Alexandraki K, Berthon A, Faucz FR, et al. Malignant pheochromocytomas/paragangliomas and ectopic hormonal secretion: a case series and review of the literature. Cancers (Basel). 2019; 11:724.
Article7. Cheng X, Zhang M, Xiao Y, Li H, Zhang Y, Ji Z. Interleukin-6-producing pheochromocytoma as a new reason for fever of unknown origin: a retrospective study. Endocr Pract. 2018; 24:507–11.
Article8. Minetto M, Dovio A, Ventura M, Cappia S, Daffara F, Terzolo M, et al. Interleukin-6 producing pheochromocytoma presenting with acute inflammatory syndrome. J Endocrinol Invest. 2003; 26:453–7.
Article9. Kang JM, Lee WJ, Kim WB, Kim TY, Koh JM, Hong SJ, et al. Systemic inflammatory syndrome and hepatic inflammatory cell infiltration caused by an interleukin-6 producing pheochromocytoma. Endocr J. 2005; 52:193–8.
Article10. Yarman S, Soyluk O, Altunoglu E, Tanakol R. Interleukin-6-producing pheochromocytoma presenting with fever of unknown origin. Clinics (Sao Paulo). 2011; 66:1843–5.
Article11. Martucci VL, Pacak K. Pheochromocytoma and paraganglioma: diagnosis, genetics, management, and treatment. Curr Probl Cancer. 2014; 38:7–41.
Article12. Ku EJ, Kim KJ, Kim JH, Kim MK, Ahn CH, Lee KA, et al. Diagnosis for pheochromocytoma and paraganglioma: a joint position statement of the Korean Pheochromocytoma and Paraganglioma Task Force. Endocrinol Metab (Seoul). 2021; 36:322–38.
Article13. Nölting S, Bechmann N, Taieb D, Beuschlein F, Fassnacht M, Kroiss M, et al. Personalized management of pheochromocytoma and paraganglioma. Endocr Rev. 2022; 43:199–239.
Article14. Gimenez-Roqueplo AP, Dahia PL, Robledo M. An update on the genetics of paraganglioma, pheochromocytoma, and associated hereditary syndromes. Horm Metab Res. 2012; 44:328–33.
Article15. van Hulsteijn LT, Dekkers OM, Hes FJ, Smit JW, Corssmit EP. Risk of malignant paraganglioma in SDHB-mutation and SDHD-mutation carriers: a systematic review and meta-analysis. J Med Genet. 2012; 49:768–76.
Article16. Benn DE, Gimenez-Roqueplo AP, Reilly JR, Bertherat J, Burgess J, Byth K, et al. Clinical presentation and penetrance of pheochromocytoma/paraganglioma syndromes. J Clin Endocrinol Metab. 2006; 91:827–36.
Article17. Boyd J, Leung AA, Sadrzadeh HS, Pamporaki C, Pacak K, Deutschbein T, et al. A high rate of modestly elevated plasma normetanephrine in a population referred for suspected PPGL when measured in a seated position. Eur J Endocrinol. 2019; 181:301–9.
Article18. Shimizu C, Kubo M, Takano K, Takano A, Kijima H, Saji H, et al. Interleukin-6 (IL-6) producing phaeochromocytoma: direct IL-6 suppression by non-steroidal anti-inflammatory drugs. Clin Endocrinol (Oxf). 2001; 54:405–10.
Article19. Fiebich BL, Lieb K, Hüll M, Berger M, Bauer J. Effects of NSAIDs on IL-1 beta-induced IL-6 mRNA and protein synthesis in human astrocytoma cells. Neuroreport. 1996; 7:1209–13.
Article20. Tung D, Ciallella J, Cheung PH, Saha S. Novel anti-inflammatory effects of doxazosin in rodent models of inflammation. Pharmacology. 2013; 91:29–34.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fuctioning Extraadrenal Paraganglioma Mimicking Acute Coronary Syndrome
- Stercoral Colitis Leading to Fatal Peritonitis and Systemic Inflammatory Response Syndrome
- Treatment of Systemic Inflammatory Response Syndrome (SIRS) Following Open Heart Surgery Developed into Shock: A case report
- A Case of Extra-adrenal Paraganglioma of the Retroperitoneum
- A Case of Systemic Inflammatory Response Syndrome Secondary to an Acute Polyarticular Gout
