Vertebro-Vertebral Fistula Occlusion Using a Woven EndoBridgeTM-Device
- Affiliations
-
- 1Department of Radiology, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 2Department of Radiology, Baylor College of Medicine, Houston, TX, USA
- 3Department of Neurosurgery, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 4Department of Neuroanaesthesiology, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- KMID: 2547283
- DOI: http://doi.org/10.5469/neuroint.2023.00430
Abstract
- Vertebro-vertebral fistulas (VVFs) are vascular lesions that may develop after trauma or spontaneously in association with connective tissue disorders. We present a rare case of a post-traumatic VVF in a young patient presenting with a painless swelling and a bruit in her left upper neck. Digital subtraction angiography showed an arteriovenous fistula between the left vertebral artery (VA) and the vertebral venous plexus with significant steal phenomenon. Endovascular therapy was performed using a Woven EndoBridgeTM (WEB)-device combined with coils that allowed preservation of the VA. The patient fully recovered from her symptoms and follow-up imaging showed stable occlusion. In conclusion, VVFs can be effectively treated using intrasaccular flow diverters such as the WEB-device, allowing for complete and stable occlusion while preserving the parent artery.
Keyword
Figure
-
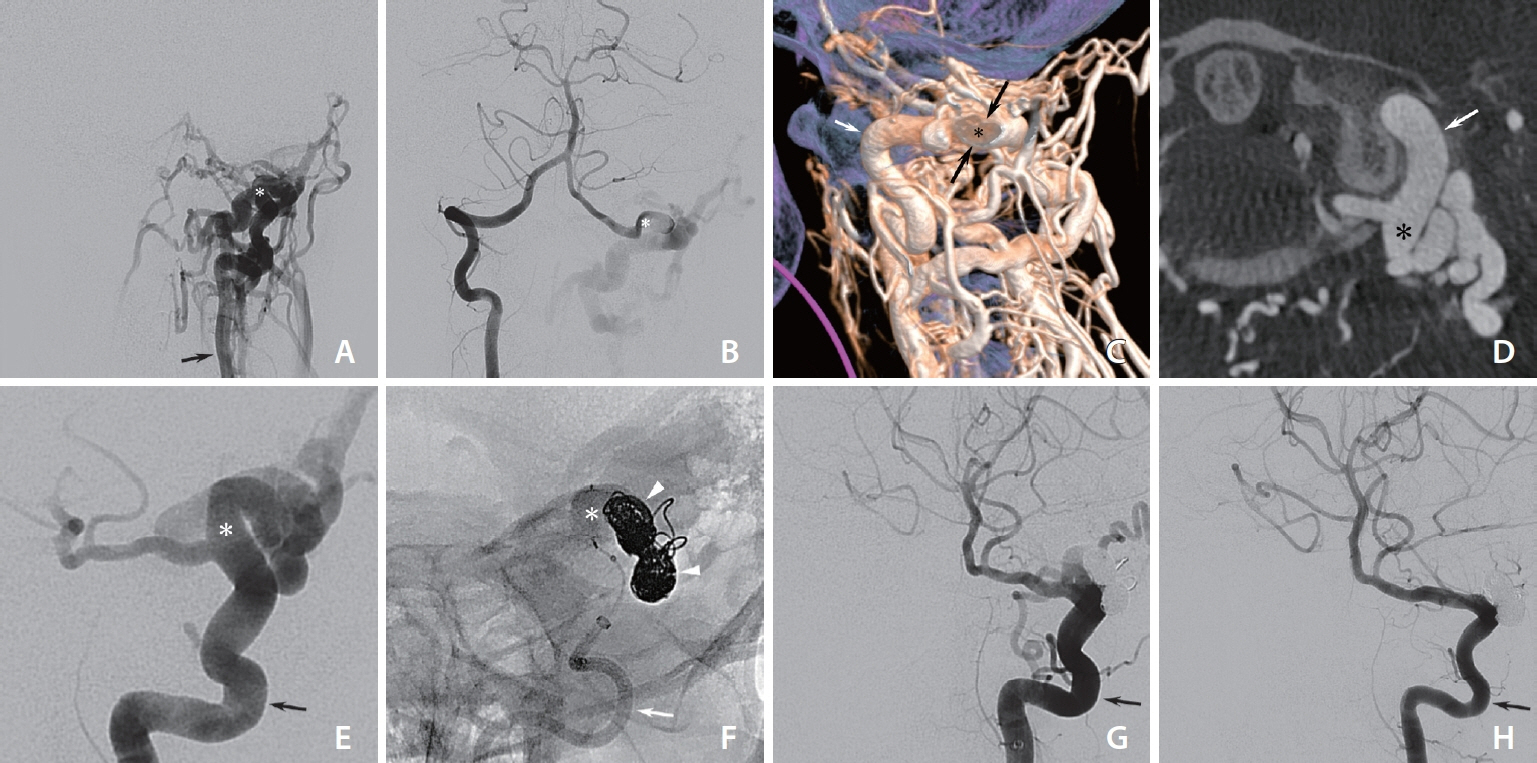
Fig. 1. (A) Left vertebral artery (VA) injection reveals a high-flow vertebro-vertebral fistula (VVF) with significant steal phenomenon and no antegrade flow in the left V4-segment. The fistulous point is marked with an asterisk. The extracranial left VA (arrow) and downstream venous system are dilated. (B) Right VA injection shows flow reversal in the left V4-segment of the VA. The fistulous point is marked with an asterisk. (C) Volume-rendered three-dimensional reconstruction from a left VA (short arrow) injection in left lateral view with a clip-plane close to the fistulous point (asterisk and long arrows). The fistulous point measured approximately 5.5 mm×6.3 mm in diameter. There is extensive filling of the vertebral venous plexus and paraspinal veins. (D) Multiplanar reconstruction of a cone-beam computed tomography with a left VA (arrow) injection shows the fistulous point (asterisk) between the V3-segment of the VA and the vertebral venous plexus. (E) Early phase left VA (arrow) injection shows the fistulous connection (asterisk) between the VA and proximal venous drainage. (F) Detachable coils (arrowheads) provided a scaffold for deployment of the Woven EndoBridgeTM-device (MicroVention) (asterisk). Catheter in the left VA (arrow). (G) Control runs with left VA (arrow) injection shows complete occlusion of the VVF. The left VA is preserved. (H) Follow-up digital subtraction angiography after 5.5 months shows persistent occlusion of the fistula. The left VA (arrow) is patent and has a normal caliber.
Cited by 1 articles
-
Intrasaccular Flow Disruptor (Woven EndoBridge) Assisted Embolization of Vertebral Arteriovenous Fistulas
Oktay Algin
Neurointervention. 2024;19(1):61-64. doi: 10.5469/neuroint.2023.00514.
Reference
-
1. Aljobeh A, Sorenson TJ, Bortolotti C, Cloft H, Lanzino G. Vertebral arteriovenous fistula: a review article. World Neurosurg. 2019; 122:e1388–e1397.
Article2. Beaujeux RL, Reizine DC, Casasco A, Aymard A, Rüfenacht D, Khayata MH, et al. Endovascular treatment of vertebral arteriovenous fistula. Radiology. 1992; 183:361–367.
Article3. Halbach VV, Higashida RT, Hieshima GB. Treatment of vertebral arteriovenous fistulas. AJR Am J Roentgenol. 1988; 150:405–412.
Article4. Benndorf G, Assmann U, Bender A, Lehmann TN, Lanksch WR. Vertebral arteriovenous fistula associated with neurofibromatosis type I misdiagnosed as a giant aneurysm. Interv Neuroradiol. 2000; 6:67–74.
Article5. Paolini S, Colonnese C, Galasso V, Morace R, Tola S, Esposito V, et al. Extradural arteriovenous fistulas involving the vertebral artery in neurofibromatosis Type 1. J Neurosurg Spine. 2008; 8:181–185.
Article6. Goyal N, Hoit D, DiNitto J, Elijovich L, Fiorella D, Pierot L, et al. How to WEB: a practical review of methodology for the use of the Woven EndoBridge. J Neurointerv Surg. 2020; 12:512–520.
Article7. Honarmand AR, Ansari SA, Alden TD, Soltanolkotabi M, Schoeneman SE, Hurley MC, et al. Endovascular management of pediatric high-flow vertebro-vertebral fistula with reversed basilar artery flow. A case report and review of the literature. Interv Neuroradiol. 2013; 19:215–221.
Article8. Briganti F, Tedeschi E, Leone G, Marseglia M, Cicala D, Giamundo M, et al. Endovascular treatment of vertebro-vertebral arteriovenous fistula. A report of three cases and literature review. Neuroradiol J. 2013; 26:339–346.
Article9. Rajadurai S, Muthukumaraswamy S, Hussain Z. Endovascular treatment of vertebral-venous fistula with flow-diverting stent. World Neurosurg. 2019; 121:33–36.
Article10. Asnafi S, Rouchaud A, Pierot L, Brinjikji W, Murad MH, Kallmes DF. Efficacy and safety of the Woven EndoBridge (WEB) device for the treatment of intracranial aneurysms: a systematic review and meta-analysis. AJNR Am J Neuroradiol. 2016; 37:2287–2292.
Article11. Tropine A, Moussa-Pacha A, Tritt S. Endovascular treatment of a direct carotid cavernous sinus fistula with the Woven EndoBridge aneurysm embolization system. Clin Neuroradiol. 2020; 30:865–867.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Woven Endobridge (WEB) augmented by Y-stent in a shallow basilar tip aneurysm
- Woven EndoBridge Device Migration and Microsnare Retrieval Strategy: Single Institutional Case Reports with Technical Video Demonstration
- Adjustment of Malpositioned Woven EndoBridge Device Using Gooseneck Snare: Complication Management Technique
- Ten Years of Clinical Evaluation of the Woven EndoBridge: A Safe and Effective Treatment for Wide-Neck Bifurcation Aneurysms
- Stent-Assisted Coil Embolization of a Vertebro-Vertebral Arteriovenous Fistula Secondary to Oriental Acupuncture: A Case Report
