Case 15: A 53-Year-Old Woman With Bilateral Leg Pain and Weakness
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 3Division of Rheumatology, Department of Internal Medicine, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 4Division of Rheumatology, Department of Internal Medicine, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2546935
- DOI: http://doi.org/10.3346/jkms.2023.38.e327
Figure
-

Fig. 1 Enhanced Lower Leg magnetic resonance imaging. Coronal (A) and axial (B) images of a contrast-enhanced magnetic resonance imaging of the lower leg showing diffuse streaky or branching hyperintensity and enhancement across both calves.

Fig. 2 The right medial gastrocnemius muscle biopsy specimen stained with hematoxylin and eosin. (A) Vasculitis accompanied by degenerated muscle fibers and lymphocytic infiltration. (B) Areas of fibrinoid necrosis (black arrow).
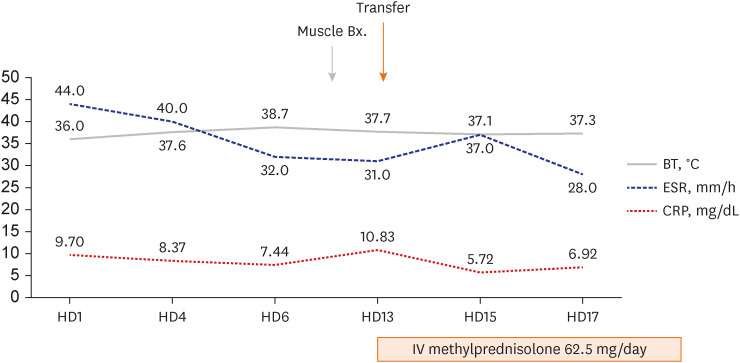
Fig. 3 Clinical progress until hospital day 17. Peak BT, serum levels of CRP, and the ESR from admission to hospital day 17. Following the confirmation of vasculitis through muscle biopsy, systemic glucocorticoid therapy was commenced on hospital day 13.BT = body temperature, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
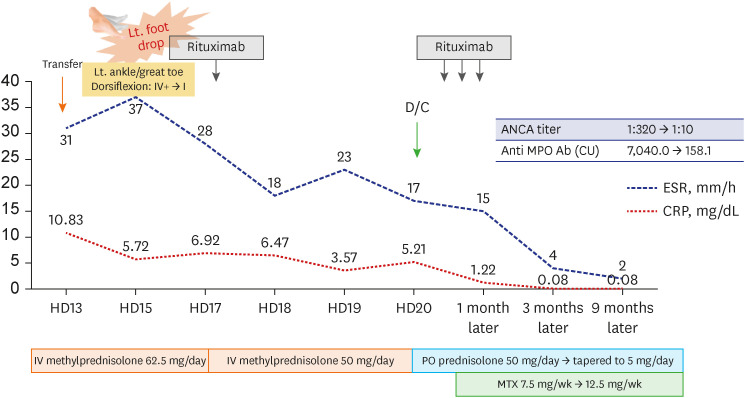
Fig. 4 Clinical progress after left foot drop occurred. The serum levels of CRP and the ESR subsequent to the occurrence of left foot drop are presented. Following the third administration of rituximab, glucocorticoid was gradually tapered, and MTX was added. Follow-up ANCA titer and anti-MPO antibody levels decreased.ANCA = antineutrophil cytoplasmic antibody, MPO = myeloperoxidase, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, HD = hospital day, IV = intravenous, MTX = methotrexate.
Reference
-
1. Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. 2007; 66(2):222–227. PMID: 16901958.2. Choi CB, Park YB, Lee SW. Antineutrophil cytoplasmic antibody-associated vasculitis in Korea: a narrative review. Yonsei Med J. 2019; 60(1):10–21. PMID: 30554486.3. Suppiah R, Robson JC, Grayson PC, Ponte C, Craven A, Khalid S, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis. Arthritis Rheumatol. 2022; 74(3):400–406. PMID: 35106973.4. Chung SA, Langford CA, Maz M, Abril A, Gorelik M, Guyatt G, et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the management of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheumatol. 2021; 73(8):1366–1383. PMID: 34235894.5. Wallace ZS, Miloslavsky EM. Management of ANCA associated vasculitis. BMJ. 2020; 368:m421. PMID: 32188597.6. Conticini E, d’Alessandro M, Al Khayyat SG, D’Alessandro R, D’Ignazio E, Pata AP, et al. Inflammatory muscle involvement in systemic vasculitis: a systematic review. Autoimmun Rev. 2022; 21(3):103029. PMID: 34971804.7. Oiwa H, Kurashige T. Muscle weakness as a presenting symptom in ANCA-associated vasculitis. Eur J Rheumatol. 2018; 5(2):139–141. PMID: 30185364.8. Nagiah S, Saranapala DM. Severe proximal muscle weakness with normal CK as a presenting feature of ANCA-associated vasculitis. BMJ Case Rep. 2020; 13(1):e232854.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Leg Weakness Caused by Bilateral Piriformis Syndrome: A Case Report
- A Case of Gait Disturbance Resolved with Hysterectomy in a Woman
- Cauda Equina Syndrome Caused by Bilateral Facet Cyst Accompanying Spinal Stenosis
- Motor Weakness on Lower Extremities after the Combined Spinal-epidural Anesthesia and Analgesia: A case report
- Multiple Hemangioendotheliomas of the Spinal Cord and Cauda Equina: Case Report
