Hepatic basidiobolomycosis masquerading as cholangiocarcinoma: a case report and literature review
- Affiliations
-
- 1Department of Pathology, SGT University, Budhera, Gurugram, India
- 2Department of Liver Transplant Surgery, Aakash Healthcare Super Speciality Hospital, Dwarka, New Delhi, India
- 3Department of Nuclear Medicine & PET-CT, Fortis Memorial Research Institute (FMRI), Gurugram, India
- 4Department of Liver Transplant Surgery, Fortis Healthcare, Budhera, Gurugram, India
- KMID: 2546418
- DOI: http://doi.org/10.17998/jlc.2023.06.07
Abstract
- Basidiobolus ranarum is known to cause subcutaneous mycoses; however, rare cases of hepatic and gastrointestinal involvement by basidiobolomycosis have been reported. Hepatic basidiobolomycosis may be confused with a carcinoma on imaging, and histological examination and fungal culture can help distinguish between these two. We report a rare case of basidiobolomycosis in a 16-year-old male with liver and gastrointestinal involvement.
Keyword
Figure
-
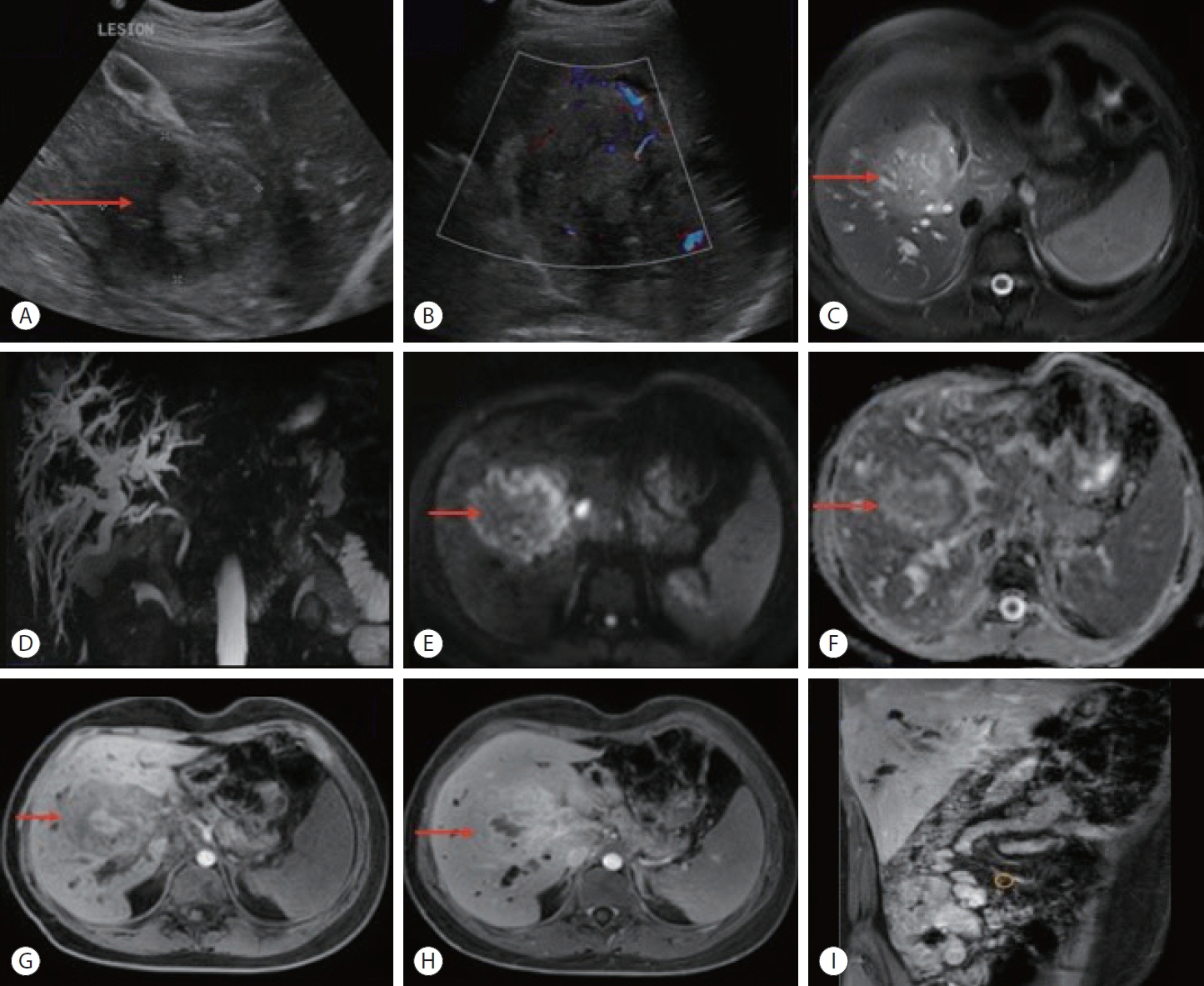
Figure 1. (A) An ultrasonography image shows a large hypoechoic lesion measuring 6.7×6.1 cm in the region of portal confluence involving segments 5, 6, and 7 of the liver (red arrow). (B) Color doppler reveals mild color flow within the lesion. (C) Transverse relaxation time fatsaturation magnetic resonance imaging of the liver demonstrates heterogeneously hyperintense signal intensity lesion (red arrow). (D) Magnetic resonance cholangiopancreatography sequence shows the mass effect with markedly dilated intrahepatic biliary radicles. (E, F) Diffusion-weighted imaging and corresponding ADC images show areas of diffusion restriction with low ADC in and around the lesion involving the right lobe of the liver (red arrows). On (G) pre- and (H) post-contrast mDIXON (T1W) studies, heterogeneous enhancement with few central non-enhancing areas was seen within the lesion (red arrows). These findings were suggestive of hilar cholangiocarcinoma. (I) Coronal post-contrast mDIXON images show thickening with an enhancement of the cecum, ascending colon, and heterogeneously enhancing lesion in the liver. ADC, apparent diffusion coefficient.

Figure 2. (A-C) Whole-body FDG positron emission tomography-computed tomography scan demonstrates FDG avid mass like ulcerated irregular thickening involving the cecum, distal ileum, and proximal ascending colon (red and black arrows) along with FDG avid paracecal lymph nodes. (D, E) A large, FDG-avid hypodense lesion showing heterogeneous post-contrast enhancement in the right lobe of the liver involving segments 5, 6, and 7 (red and black arrows) measuring approximately 7.0×8.0×6.4 cm in size. FDG, fluorodeoxyglucose.

Figure 3. Liver biopsy shows mainly fibrocollagenous tissue with inflammatory infiltrate and granulomatous reaction. Fungal spores are noted within giant cells. (A) H&E (×4), (B) H&E (×10), and (C) H&E (×20). H&E, hematoxylin and eosin.

Figure 4. (A, B) Colonoscopy shows deformed, edematous ascending colon and cecum along with deep ulcers in the colon (measuring up to 1 cm in diameter).
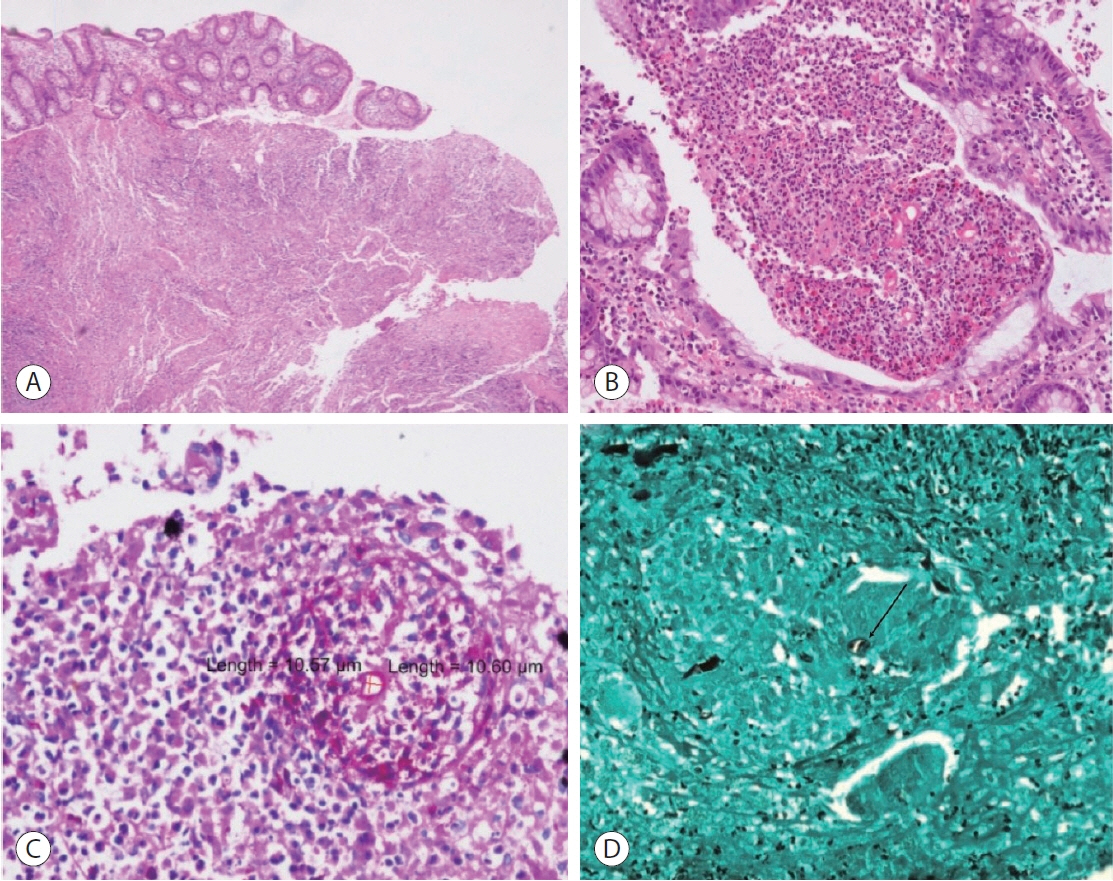
Figure 5. Section from colonic tissue biopsy shows an area of ulceration and a dense infiltrate of eosinophils. Splendore-Hoeppli phenomenon noted around fungal spores. (A) H&E (×4), (B) H&E (×10). Periodic acid-Schiff (PAS) and Grocott methenamine silver (GMS) stains show fungal spores (black arrow) with Splendore-Hoeppli phenomenon. (C) PAS (×20), (D) GMS (×10). H&E, hematoxylin and eosin.
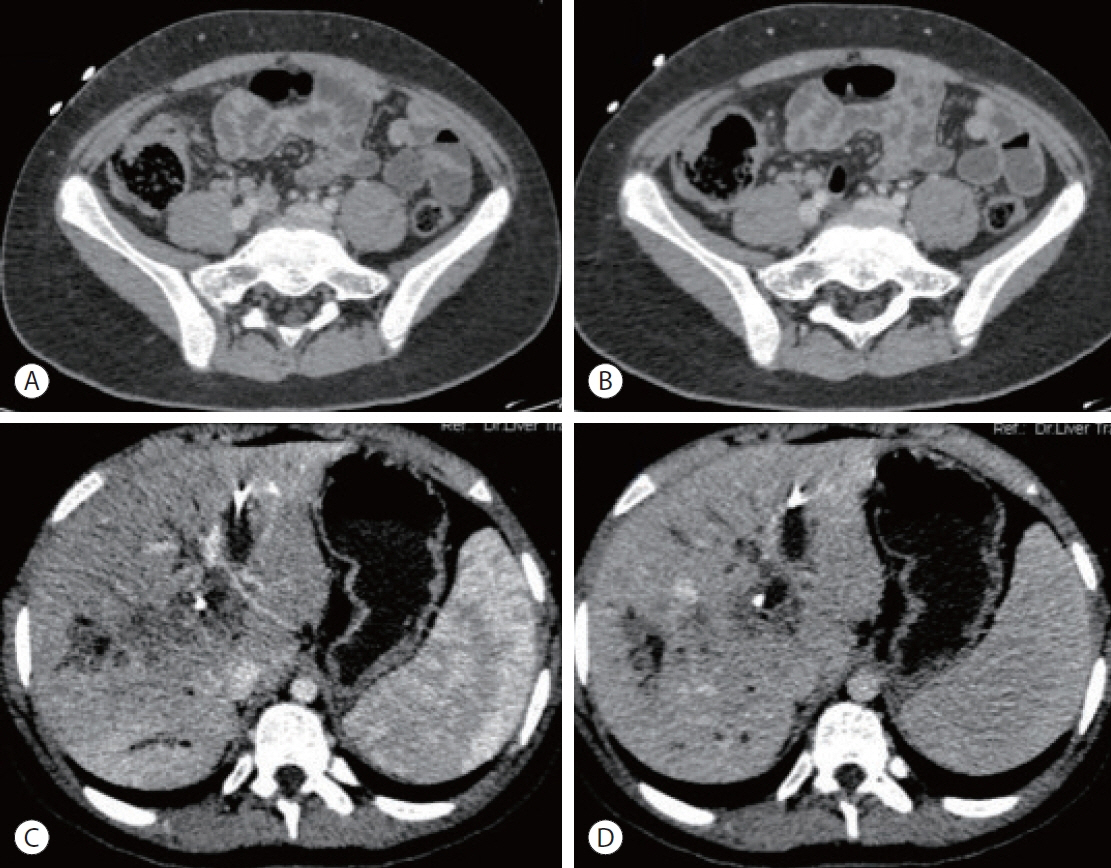
Figure 6. (A, B) The triphasic follow-up contrast-enhanced computed tomography scan demonstrates interval resolution of the irregular, ileocecal thickening and paracecal lymph nodes (porto-venous phase). (C) Arterial, (D) porto-venous phase. There was an interval reduction in the size of the liver lesions.
Reference
-
References
1. Hussein MRA, Alqahtani AS, Alhagawi Y, Al Saglan NS, Albishi AM, Ahmed FO, et al. Primary basidiobolomycosis of the cecum in immunocompetent patients: two case reports. Gastroenterology Res. 2021; 14:116–124.2. Gugnani HC. A review of zygomycosis due to Basidiobolus ranarum. Eur J Epidemiol. 1999; 15:923–929.3. Lyon GM, Smilack JD, Komatsu KK, Pasha TM, Leighton JA, Guarner J, et al. Gastrointestinal basidiobolomycosis in Arizona: clinical and epidemiological characteristics and review of the literature. Clin Infect Dis. 2001; 32:1448–1455.4. Elzein F, Mursi M, Albarrag AM, Alfiaar A, Alzahrani A. Disseminated angioinvasive basidiobolomycosis with a favourable outcome. Med Mycol Case Rep. 2018; 22:30–34.5. Takrouni AO, Schammut MH, Al-Otaibi M, Al-Mulla M, Privitera A. Disseminated intestinal basidiobolomycosis with mycotic aneurysm mimicking obstructing colon cancer. BMJ Case Rep. 2019; 12:e225054.6. Gopinath D. Splendore-Hoeppli phenomenon. J Oral Maxillofac Pathol. 2018; 22:161–162.7. Abduh MS, Aldaqal SM, Almaghrabi J, Aljiffry MM, Elbadrawy HA, Alsahafi MA. A very rare basidiobolomycosis case presented with cecal perforation and concomitant hepatic involvement in an elderly male patient: a case study. Int J Environ Res Public Health. 2022; 19:3412.8. Jafarpour Z, Pouladfar G, Dehghan A, Anbardar MH, Foroutan HR. Case report: gastrointestinal basidiobolomycosis with multi-organ involvement presented with intussusception. Am J Trop Med Hyg. 2021; 105:1222–1226.9. Dashti AS, Nasimfar A, Khorami HH, Pouladfar G, Kadivar MR, Geramizadeh B, et al. Gastro-intestinal basidiobolomycosis in a 2-year-old boy: dramatic response to potassium iodide. Paediatr Int Child Health. 2018; 38:150–153.10. Zekavat OR, Abdolkarimi B, Pouladfar G, Fathpour G, Mokhtari M, Shakibazad N. Colonic basidiobolomycosis with liver involvement masquerading as gastrointestinal lymphoma: a case report and literature review. Rev Soc Bras Med Trop. 2017; 50:712–714.11. Geramizadeh B, Dashti AS, Kadivar MR, Kord S. Isolated hepatic basidiobolomycosis in a 2-year-old girl: the first case report. Hepat Mon. 2015; 15:e30117.12. Flicek KT, Vikram HR, De Petris GD, Johnson CD. Abdominal imaging findings in gastrointestinal basidiobolomycosis. Abdom Imaging. 2015; 40:246–250.13. Ejtehadi F, Anushiravani A, Bananzadeh A, Geramizadeh B. Gastrointestinal basidiobolomycosis accompanied by liver involvement: a case report. Iran Red Crescent Med J. 2014; 16:e14109.14. Saeed MA, Al Khuwaitir TS, Attia TH. Gastrointestinal basidiobolomycosis with hepatic dissemination: a case report. JMM Case Rep. 2014; 1:e003269.15. Hassan HA, Majid RA, Rashid NG, Nuradeen BE, Abdulkarim QH, Hawramy TA, et al. Eosinophilic granulomatous gastrointestinal and hepatic abscesses attributable to basidiobolomycosis and fasciolias: a simultaneous emergence in Iraqi Kurdistan. BMC Infect Dis. 2013; 13:91.16. Al-Shanafey S, AlRobean F, Bin Hussain I. Surgical management of gastrointestinal basidiobolomycosis in pediatric patients. J Pediatr Surg. 2012; 47:949–951.17. van den Berk GE, Noorduyn LA, van Ketel RJ, van Leeuwen J, Bemelman WA, Prins JM. A fatal pseudo-tumour: disseminated basidiobolomycosis. BMC Infect Dis. 2006; 6:140.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary hepatic tuberculosis mimicking intrahepatic cholangiocarcinoma: report of two cases
- Intrahepatic Cholangiocarcinoma Initially Presented as a Distant Metastatic Lymph Node without Demonstrable Hepatic Mass: A Case Report
- Primary Cholangiocarcinoma of the Liver Presenting as a Complicated Hepatic Cyst: A Diagnostic Challenge
- Subcutaneous Basidiobolomycosis: A Rare and Underdiagnosed but Curable Fungal Infection -A Case Report
- MR Features of Common Hepatic Duct Cholangiocarcinoma
