Reconstruction of a skull base defect with cutaneous nasocranial communication using a combination of an anterolateral thigh free flap and galeal flap division: a case report
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2545531
- DOI: http://doi.org/10.12790/ahm.23.0019
Abstract
- Soft tissue defects can occur in the head and neck due to various causes, and head and neck surgery is often performed to reconstruct soft tissue defects. However, head and neck reconstruction remains delicate and complex as a surgical procedure. The reconstruction of a large defect at the base of the skull, especially after resection of cancer in the anterior base of the skull that has invaded adjacent tissues, is particularly difficult. We present a case of successful reconstruction of a large skull base defect using an anterolateral thigh (ALT) free flap and galeal flap division after tumor resection in the anterior skull base. Paranasal sinus cancer involving the bilateral frontoethmoidal sinuses was resected, and an anterior skull base defect was noted, with communication between the intracranium and nasal cavity and a skin defect at the glabella. A galeal flap was divided to create an anatomical and functional barrier to communication between the nasal cavity and intracranium. The soft tissue defect at the anterior skull base was then reconstructed using an ALT free flap containing the vastus lateralis muscle, and the skin defect at the glabella was covered. No postoperative complications, such as cerebrospinal fluid leakage, developed. The reconstructed flap remained intact after subsequent radiation therapy. Based on this study, we propose that using a galeal flap and ALT free flap in a large skull base defect can yield a robust flap that can endure postoperative radiotherapy with a minimal risk of complications.
Keyword
Figure
-

Fig. 1. Preoperative magnetic resonance imagings (MRIs). A malignant soft tissue mass involving the bilateral fronto-ethmoidal sinuses, with adjacent bony erosion, was proven to be paranasal sinus cancer. It extended to the overlying subcutaneous tissue of the dorsum of the nose. (A) Coronal view of the patient's MRI. (B) Sagittal view of the patient's MRI. (C) Axial view of the patient's MRI. (D) Axial view of the patient's MRI. Suspicious focal dural involvement was noted in the lateral aspect of the right lateral orbital gyrus (arrow).
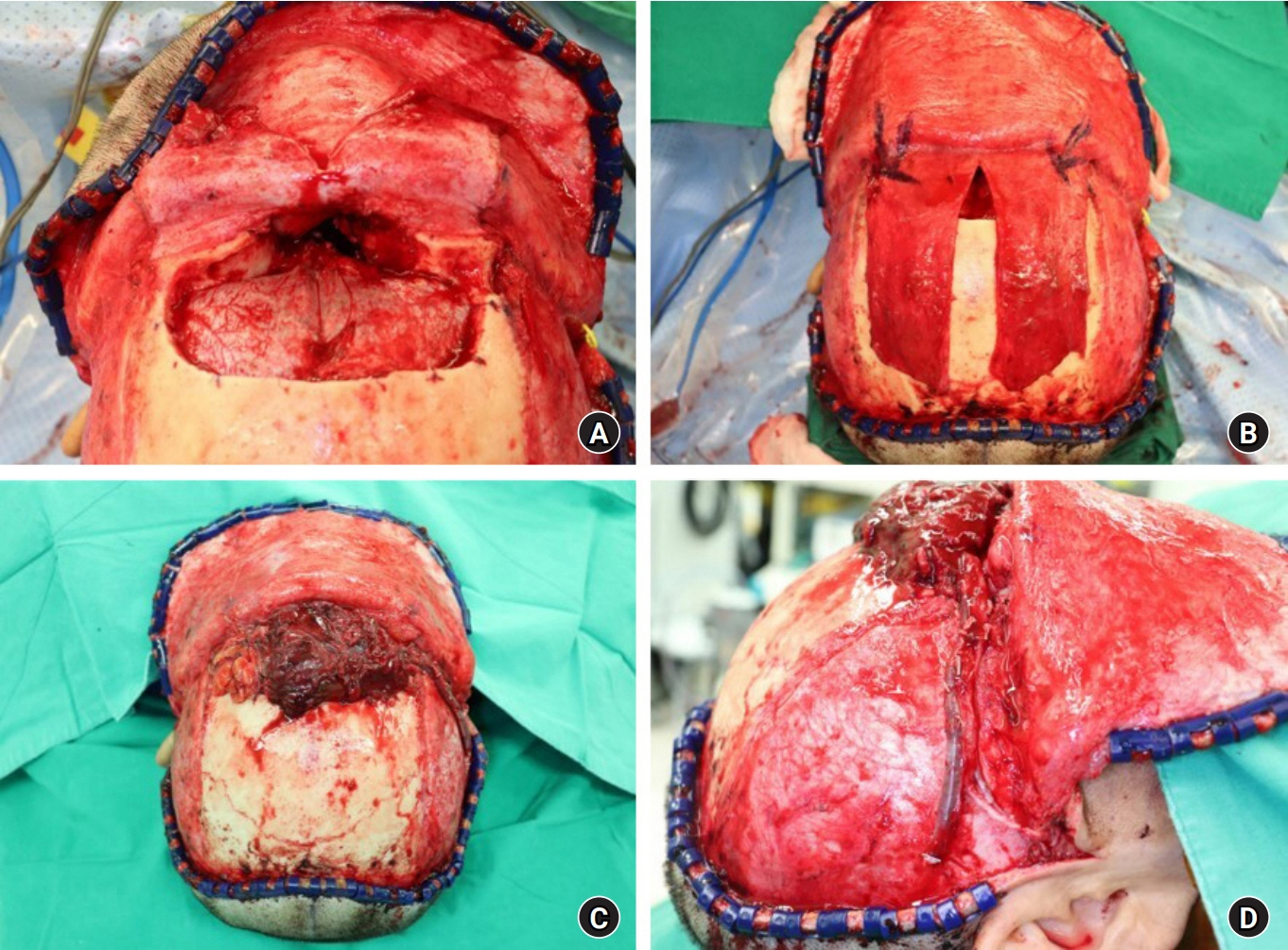
Fig. 2. Photographs of the intraoperative procedure. (A) The defect of the anterior skull base after resection of the tumor, with communication between the intracranial cavity and the nasal cavity. (B) The divided galeal flap, which was designed to create an anatomical and functional barrier to communication between the intracranial cavity and the nasal cavity. (C) Photograph of the harvested anterolateral thigh free flap covering the frontal skull base defect. (D) Photograph of the microanastomosis performed. (donor: descending branch of the lateral circumflex femoral artery and venae comitantes; recipient: left superficial temporal artery, venae comitantes, and occipital vein).

Fig. 3. Immediate postoperative photographs.

Fig. 4. Postoperative photographs of the patient after 10 months.
Reference
-
References
1. Palade DO, Hainarosie R, Pertea M, et al. Reconstructive challenges of sinonasal tumors: a case report. Exp Ther Med. 2022; 23:419.
Article2. Bridger GP, Kwok B, Baldwin M, Williams JR, Smee RI. Craniofacial resection for paranasal sinus cancers. Head Neck. 2000; 22:772–80.
Article3. Gorelick J, Ross D, Marentette L, Blaivas M. Sinonasal undifferentiated carcinoma: case series and review of the literature. Neurosurgery. 2000; 47:750–5.
Article4. Gil Z, Abergel A, Leider-Trejo L, et al. A comprehensive algorithm for anterior skull base reconstruction after oncological resections. Skull Base. 2007; 17:25–37.
Article5. Yano T, Tanaka K, Kishimoto S, Iida H, Okazaki M. Reliability of and indications for pericranial flaps in anterior skull base reconstruction. J Craniofac Surg. 2011; 22:482–5.
Article6. Eloy JA, Choudhry OJ, Christiano LD, Ajibade DV, Liu JK. Double flap technique for reconstruction of anterior skull base defects after craniofacial tumor resection: technical note. Int Forum Allergy Rhinol. 2013; 3:425–30.
Article7. Nameki H, Kato T, Nameki I, Ajimi Y. Selective reconstructive options for the anterior skull base. Int J Clin Oncol. 2005; 10:223–8.
Article8. Ein L, Sargi Z, Nicolli EA. Update on anterior skull base reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2019; 27:426–30.
Article9. Moyer JS, Chepeha DB, Teknos TN. Contemporary skull base reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2004; 12:294–9.
Article10. Wang W, Vincent A, Sokoya M, Kohlert S, Kadakia S, Ducic Y. Free-flap reconstruction of skull base and orbital defects. Semin Plast Surg. 2019; 33:72–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extended temporalis flap for skull base reconstruction
- Total Tongue Reconstruction with Folded Anterolateral Thigh Free Flap
- Reconstruction of the Tissue Defects of Extremities with Anterolateral Thigh Free Flap
- Anterior skull base reconstruction using an anterolateral thigh free flap
- Reconstruction of Tissue Defects with Anterolateral Thigh Sensate Free Flap
