Entero-colonic Fistula Secondary to Necrotizing Enterocolitis in Premature Infant: A Case Report
- Affiliations
-
- 1Department of Radiology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
- KMID: 2545430
- DOI: http://doi.org/10.5385/nm.2023.30.3.83
Abstract
- Necrotizing enterocolitis is a severe inflammatory disease of the intestine and is the main cause of death in infants, mostly occurring in premature infants. Intestinal obstruction may occur during the medical treatment of necrotizing enterocolitis. A common cause of intestinal obstruction is intestinal stricture, and entero-enteric fistulas may form in the proximal portion of the intestinal stricture. Several mechanisms may be suggested for the development of entero-enteric fistula. Intestinal ischemia and subsequent necrosis do not become intestinal perforation over time, causing an inflammatory reaction, and are attached to the adjacent intestine, forming a fistula. Alternatively, a subacute perforation may be sealed off by the adjacent intestine, resulting in fistula formation. Entero-enteric fistulas are closely related to distal stricture and occurs when there is a localized perforation rather than a generalized perforation. Fistulas can be diagnosed via contrast enema examination or distal loopogram, and surgical resection is required. Here, I report a case of a preterm infant with an entero-colonic fistula secondary to necrotizing enterocolitis. The patient had abdominal distention and bloody stool and was confirmed to have rotavius enteritis. Plain abdominal radiographs showed pneumatosis intestinalis. The patient received medical treatment for necrotizing enterocolitis. While the symptoms were improving, he vomited again, and intestinal obstruction was suspected. Gastrografin enema was performed due to intestinal obstruction, and an enterocolonic fistula was found.
Keyword
Figure
-
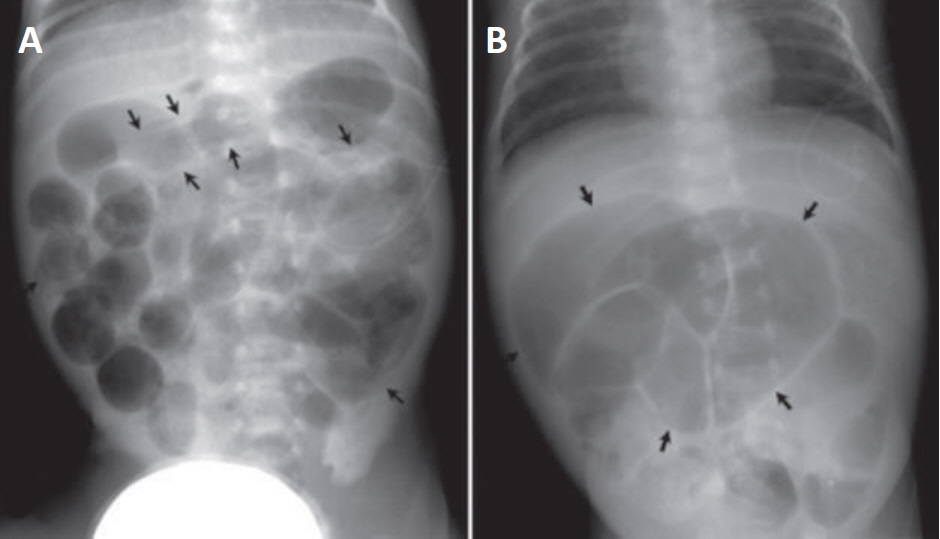
Figure 1. (A) Plain abdominal radiograph taken at hospital day 8, shows multiple dilated bowel loops throughout the abdomen. Linear bands of radiolucency that are parallel to the bowel wall are noted, which indicate pneumatosis intestinalis (arrows). (B) Plain abdominal radiograph taken at hospital day 51, shows dilated small bowels (arrows) in upper abdomen and paucity of colonic gas, suggesting intestinal obstruction.
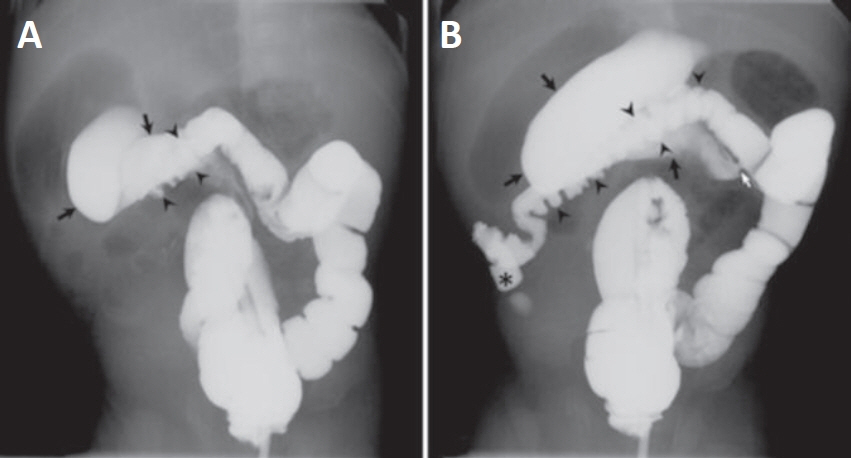
Figure 2. Gastrografin enema examination taken at hospital day 52. (A) Part of the transverse colon (arrowheads) is opacified with contrast media and the ascending colon is not yet visible, but the small bowel (black arrows) is filled with contrast media. (B) Fistula (white arrow) is noted between the transverse colon and the jejunum. Transverse colon (arrowheads) and ascending colon (asterisk) are collapsed, but the small bowel (black arrows) is dilated. Considering that the small bowel filled with contrast media is dilated, it can be assumed that the obstruction is more distal than visible small bowel.
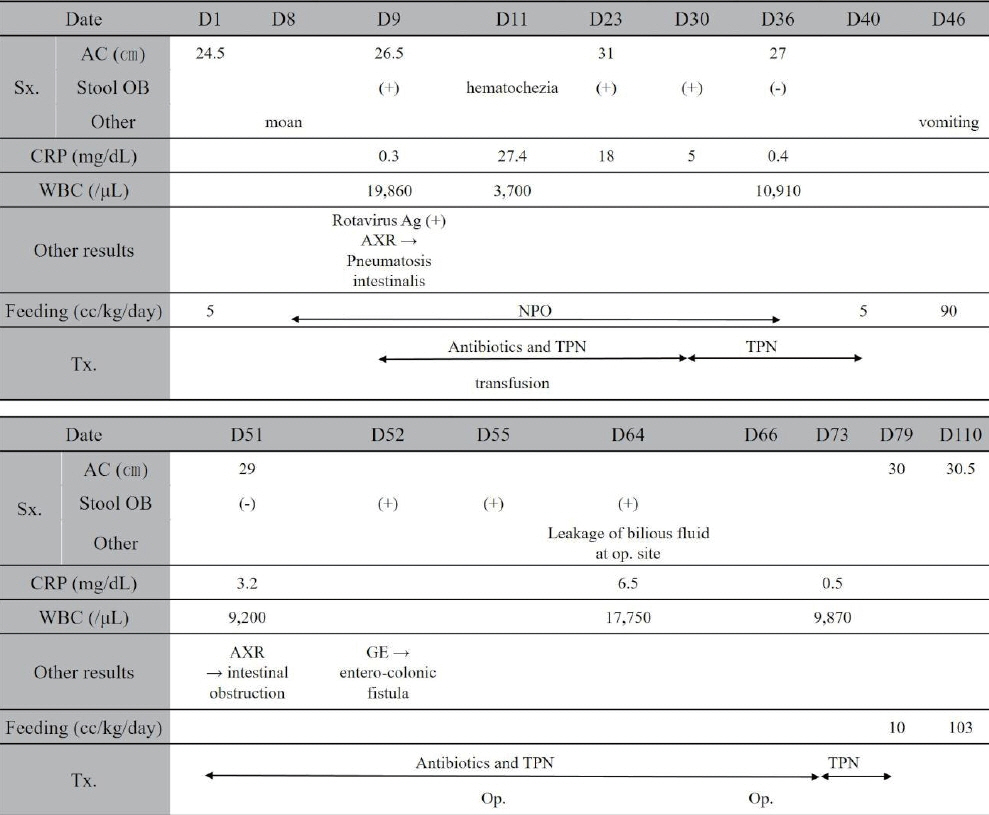
Figure 3. Clinical course of patient. Abbreviations: D, hospital day; Sx., symptom; AC, abdominal circumference; OB, occult blood; CRP, C-reactive protein; WBC, white blood cell count; Ag, antigen; AXR, abdominal X-ray; NPO, nothing per oral; Tx, treatment; TPN, total parenteral nutrition; Op., operation; GE, gastrografin enema.
Reference
-
1. Yee WH, Soraisham AS, Shah VS, Aziz K, Yoon W, Lee SK, et al. Incidence and timing of presentation of necrotizing enterocolitis in preterm infants. Pediatrics. 2012; 129:e298–304.2. Pierro A. The surgical management of necrotising enterocolitis. Early Hum Dev. 2005; 81:79–85.3. Nam SH, Kim DY, Kim SC, Kim IK. The experience of surgical treatment of necrotizing enterocolitis. J Korean Surg Soc. 2009; 76:246–51.4. Stringer MD, Cave E, Puntis JW, Beck JM, Arthur RJ. Enteric fistulas and necrotizing enterocolitis. J Pediatr Surg. 1996; 31:1268–71.5. Kiely E, Eckstein HB. Colonic stricture and enterocolic fistulae following necrotizing enterocolitis. Br J Surg. 1984; 71:613.6. Paley RH, McCarten KM, Cleveland RH. Enterocolonic fistula as a late complication of necrotizing enterocolitis. AJR Am J Roentgenol. 1979; 132:989–90.7. Dwight P, Poenaru D. Entero-enteric fistula following mild necrotizing enterocolitis. Eur J Pediatr Surg. 2005; 15:137–9.8. Levin TL, Brill PW, Winchester P. Enteric fistula formation secondary to necrotizing enterocolitis. Pediatr Radiol. 1991; 21:309–11.9. Walsh MC, Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am. 1986; 33:179–201.10. Choi YY. Necrotizing enterocolitis in newborns: update in pathophysiology and newly emerging therapeutic strategies. Korean J Pediatr. 2014; 57:505–13.11. Choi EK, Kim H, Choi JY, Kim S, Jung E, Lee J, et al. Three cases of preterm infants showing pneumatosis intestinalis without progression to typical necrotizing enterocolitis. Neonatal Med. 2014; 21:192–7.12. Abdullah F, Zhang Y, Camp M, Mukherjee D, Gabre-Kidan A, Colombani PM, et al. Necrotizing enterocolitis in 20,822 infants: analysis of medical and surgical treatments. Clin Pediatr (Phila). 2010; 49:166–71.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Necrotizing Enterocolitis Associated with Norovirus Infection in a Preterm Infant
- Food Protein-induced Enterocolitis Mimic king Necrotizing Enterocolitis in a Premature Infant: Case Report
- Two Cases of Necrotizing Enterocolitis Associated with Rotavirus Infection in Premature Infants
- Idiopathic Pneumoperitoneum in a Premature Infant
- Multiple Intussusceptions in an Extremely Premature Infant
