Intrarenal Mechanisms of Sodium-Glucose Cotransporter-2 Inhibitors on Tubuloglomerular Feedback and Natriuresis
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Division of Nephrology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
- KMID: 2545268
- DOI: http://doi.org/10.3803/EnM.2023.1764
Abstract
- When sodium-glucose cotransporter-2 (SGLT2) inhibitors were first introduced a decade ago, no one expected them to have substantial effects beyond their known glucose-lowering effects, until the emergence of evidence of their robust renal and cardiovascular benefits showing that they could attenuate progression of kidney disease, irrespective of diabetes, as well as prevent the development of acute kidney injury. Still, the precise and elaborate mechanisms underlying the major organ protection of SGLT2 inhibitors remain unclear. SGLT2 inhibitors inhibit the reabsorption of sodium and glucose in the proximal tubule of the kidney and then recovers tubuloglomerular feedback, whereby SGLT2 inhibitors reduce glomerular hyperfiltration. This simple demonstration of their beneficial effects has perplexed experts in seeking more plausible and as yet undisclosed explanations for the whole effects of SGLT2 inhibitors, including metabolism reprogramming and the modulation of hypoxia, inflammation, and oxidative stress. Given that the renal benefits of SGLT2 inhibitors in patients with kidney disease but without diabetes were comparable to those seen in patients with diabetes, it may be reasonable to keep the emphasis on their hemodynamic actions. In this context, the aim of the present review is to provide a comprehensive overview of renal hemodynamics in individuals with diabetes who are treated with SGLT2 inhibitors, with a focus on natriuresis associated with the regulation of tubuloglomerular feedback and potential aquaresis. Throughout the discussion of alterations in renal sodium and water transports, particular attention will be given to the potential enhancement of adenosine and its receptors following SGLT2 inhibition.
Keyword
Figure
-
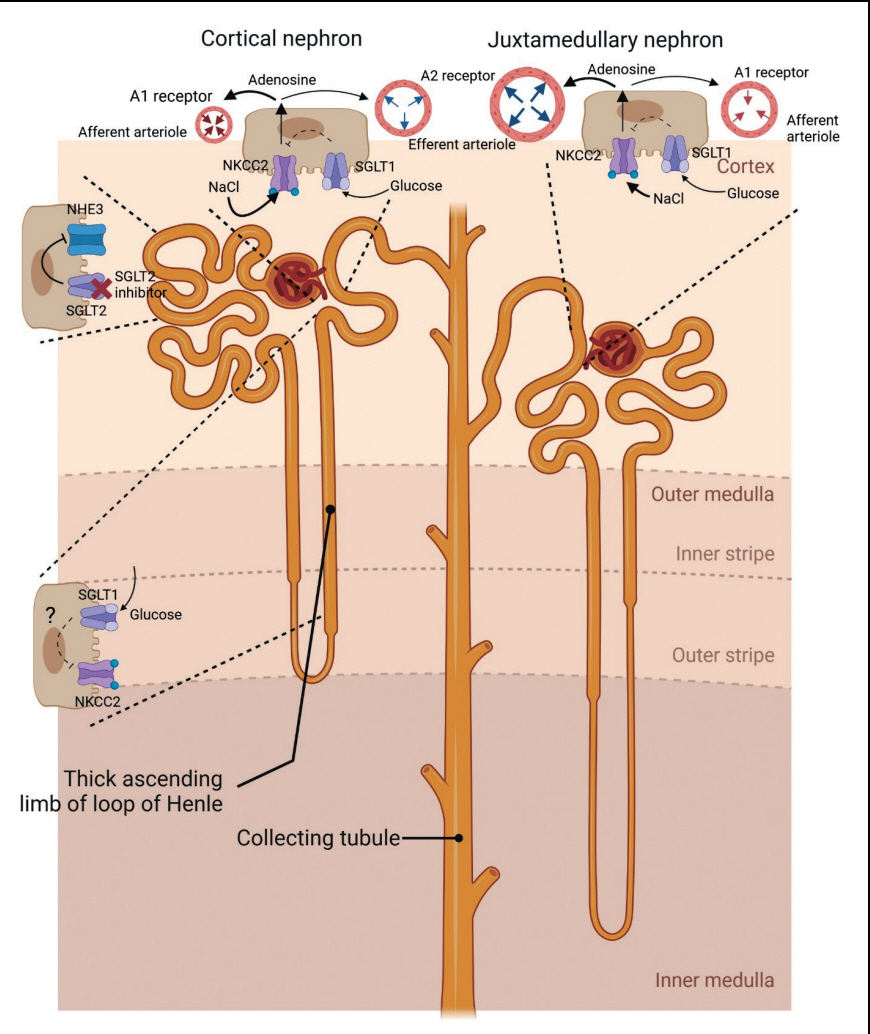
Fig. 1. Proposed effects of sodium-glucose contrasnporter-2 (SGLT2) inhibitors on tubular transports in proximal nephron. In diabetic condition, the expression of SGLT2 is increased with exposure to the increased glycosuria, and then SGLT2 in diabetes accounts for more Na reabsorption than usual in normal status. SGLT2 inhibitors increase the distal delivery of sodium chloride (NaCl) by inhibiting SGLT2 as well as decreasing sodium–hydrogen exchanger 3 (NHE3) activity (which may not be a specific action of SGLT2 inhibitors). Sodium-glucose contrasnporter-1 (SGLT1) is expressed on the thick ascending limb of the loop of Henle, the macula densa, and the proximal tubule. The increased luminal glucose resulting from SGLT2 inhibition may be reabsorbed via SGLT1 on the thick ascending limb and the macula densa, and it may then repress upregulation of Na+-K+-2Cl− cotransporter (NKCC2). In macula densa, the increase in luminal NaCl concentration is sensed by NKCC2, causing the release of adenosine from macula densa, and then affecting arterioles. This process may be subject to check by SGLT1 activity stimulated by the increased luminal glucose concentration. The adenosine released from macula densa can act as a vasoconstrictor in afferent arteriole and vasodilator in efferent arteriole by binding A1 receptor and A2 receptor respectively. Responding to high adenosine concentrations, adenosine A1 receptor-mediated afferent arteriolar constriction may dominate in cortical nephrons, while adenosine A2 receptor-mediated vasodilatation may be more dominant in juxtamedullary or deep cortical nephrons. Under any location of the nephron, the final outcome of SGLT2 inhibitors is a reduction of intraglomerular pressure.
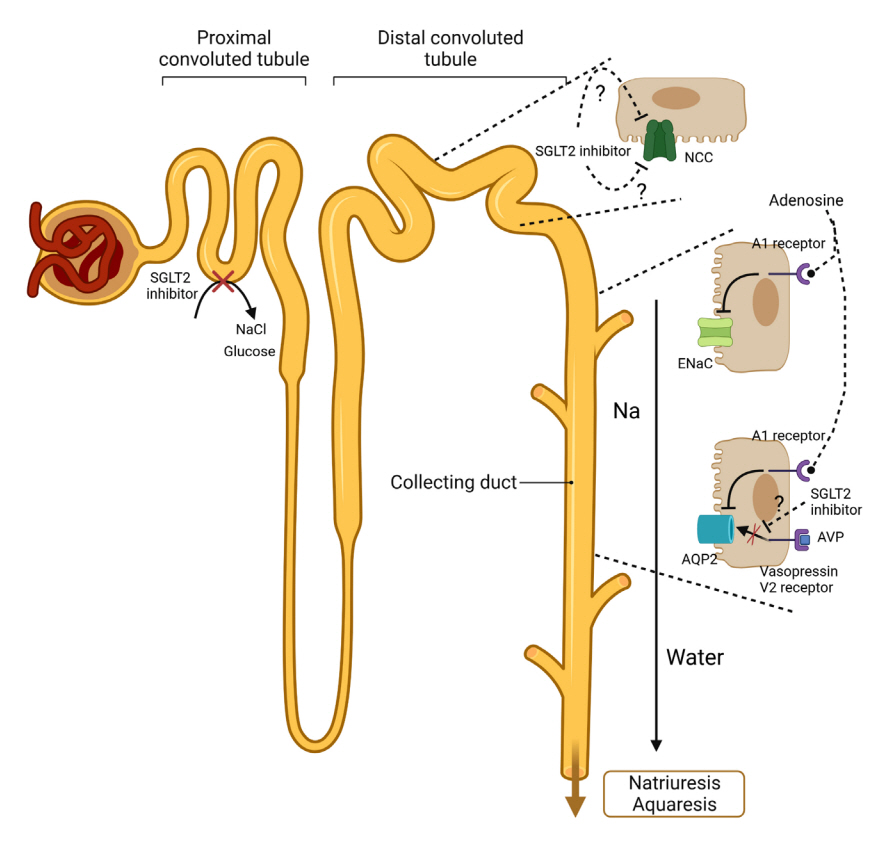
Fig. 2. Proposed effects of sodium-glucose contrasnporter-2 (SGLT2) inhibitors on tubular transports in distal nephron. The treatment with SGLT2 inhibitors cause a decrease in sodium chloride cotransporter (NCC) levels by not-yet-identified mechanisms. Despite some conflicting results, the expression epithelial sodium channel (ENaC) γ-subunit is decreased by SGLT2 inhibitors. The interstitial adenosine, released from macula densa, could inhibit ENaC activity by activating adenosine A1 receptors in the collecting duct. The increased interstitial adenosine could also suppress aquaporin-2 (AQP2) in collecting duct by binding the adenosine A1 receptor and disrupting signaling pathways between vasopressin V2 receptor and AQP2 synthesis. Collectively, disturbed Na reabsorption in various tubules and decreased water reabsorption in distal nephron by SGLT2 inhibitors could lead to natriuresis and aquaresis. AVP, arginine vasopressin.
Cited by 1 articles
-
Chronic Kidney Disease and SGLT2 Inhibitors
Eun Sil Koh, Sungjin Chung
J Korean Diabetes. 2024;25(1):16-25. doi: 10.4093/jkd.2024.25.1.16.
Reference
-
1. Garibotto G, Picciotto D, Esposito P. Treatment of chronic kidney disease: moving forward. J Clin Med. 2022; 11:6948.2. Hong YA, Ban TH, Kang CY, Hwang SD, Choi SR, Lee H, et al. Trends in epidemiologic characteristics of end-stage renal disease from 2019 Korean Renal Data System (KORDS). Kidney Res Clin Pract. 2021; 40:52–61.3. Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022; 12:7–11.4. Mills KT, Xu Y, Zhang W, Bundy JD, Chen CS, Kelly TN, et al. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015; 88:950–7.5. Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases. Nephrol Dial Transplant. 2019; 34:1803–5.6. Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018; 392:2052–90.7. Inrig JK, Califf RM, Tasneem A, Vegunta RK, Molina C, Stanifer JW, et al. The landscape of clinical trials in nephrology: a systematic review of Clinicaltrials.gov. Am J Kidney Dis. 2014; 63:771–80.8. Breyer MD, Susztak K. Developing treatments for chronic kidney disease in the 21st century. Semin Nephrol. 2016; 36:436–47.9. Tuttle KR, McGill JB, Haney DJ, Lin TE, Anderson PW; PKC-DRS, PKC-DMES, and PKC-DRS 2 Study Groups. Kidney outcomes in long-term studies of ruboxistaurin for diabetic eye disease. Clin J Am Soc Nephrol. 2007; 2:631–6.10. Mann JF, Green D, Jamerson K, Ruilope LM, Kuranoff SJ, Littke T, et al. Avosentan for overt diabetic nephropathy. J Am Soc Nephrol. 2010; 21:527–35.11. Sharma K, Ix JH, Mathew AV, Cho M, Pflueger A, Dunn SR, et al. Pirfenidone for diabetic nephropathy. J Am Soc Nephrol. 2011; 22:1144–51.12. Packham DK, Wolfe R, Reutens AT, Berl T, Heerspink HL, Rohde R, et al. Sulodexide fails to demonstrate renoprotection in overt type 2 diabetic nephropathy. J Am Soc Nephrol. 2012; 23:123–30.13. Parving HH, Brenner BM, McMurray JJ, de Zeeuw D, Haffner SM, Solomon SD, et al. Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med. 2012; 367:2204–13.14. de Zeeuw D, Akizawa T, Audhya P, Bakris GL, Chin M, Christ-Schmidt H, et al. Bardoxolone methyl in type 2 diabetes and stage 4 chronic kidney disease. N Engl J Med. 2013; 369:2492–503.15. Mark PB, Sattar N. Implementation, not hesitation, for SGLT2 inhibition as foundational therapy for chronic kidney disease. Lancet. 2022; 400:1745–7.16. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015; 373:2117–28.17. Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016; 375:323–34.18. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023; 388:117–27.19. Nuffield Department of Population Health Renal Studies Group; SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists’ Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet. 2022; 400:1788–801.20. Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020; 98(4S):S1–115.21. Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2022; 102(5S):S1–127.22. Clinical Practice Guideline Committee of the Korean Society of Nephrology. Korean Society of Nephrology 2023 practical recommendations for the management of diabetic kidney disease. [Internet]. Seoul: Korean Society of Nephrology;2023. [cited 2023 Jul 11]. Available from: https://ksn.or.kr/bbs/?code=guideline_k.23. Watanabe K, Sato E, Mishima E, Miyazaki M, Tanaka T. What’s new in the molecular mechanisms of diabetic kidney disease: recent advances. Int J Mol Sci. 2022; 24:570.24. Hahn K, Ejaz AA, Kanbay M, Lanaspa MA, Johnson RJ. Acute kidney injury from SGLT2 inhibitors: potential mechanisms. Nat Rev Nephrol. 2016; 12:711–2.25. Chung S, Kim GH. Use of anti-diabetic agents in non-diabetic kidney disease: from bench to bedside. Life (Basel). 2021; 11:389.26. Zatz R, Meyer TW, Rennke HG, Brenner BM. Predominance of hemodynamic rather than metabolic factors in the pathogenesis of diabetic glomerulopathy. Proc Natl Acad Sci U S A. 1985; 82:5963–7.27. Ellison DH. SGLT2 inhibitors, hemodynamics, and kidney protection. Am J Physiol Renal Physiol. 2021; 321:F47–9.28. Palmer LG, Schnermann J. Integrated control of Na transport along the nephron. Clin J Am Soc Nephrol. 2015; 10:676–87.29. Thomson SC, Vallon V. Renal effects of sodium-glucose co-transporter inhibitors. Am J Cardiol. 2019; 124(Suppl 1):S28–35.30. Gronda E, Vanoli E, Iacoviello M, Caldarola P, Gabrielli D, Tavazzi L. The benefit of sodium-glucose co-transporter inhibition in heart failure: the role of the kidney. Int J Mol Sci. 2022; 23:11987.31. Poursharif S, Hamza S, Braam B. Changes in proximal tubular reabsorption modulate microvascular regulation via the TGF system. Int J Mol Sci. 2022; 23:11203.32. Thomson SC, Blantz RC. Glomerulotubular balance, tubuloglomerular feedback, and salt homeostasis. J Am Soc Nephrol. 2008; 19:2272–5.33. Brochner-Mortensen J, Stockel M, Sorensen PJ, Nielsen AH, Ditzel J. Proximal glomerulo-tubular balance in patients with type 1 (insulin-dependent) diabetes mellitus. Diabetologia. 1984; 27:189–92.34. Takenaka T, Inoue T, Watanabe Y. How the kidney hyperfiltrates in diabetes: from molecules to hemodynamics. World J Diabetes. 2015; 6:576–82.35. Takenaka T, Inoue T, Ohno Y, Miyazaki T, Nishiyama A, Ishii N, et al. Elucidating mechanisms underlying altered renal autoregulation in diabetes. Am J Physiol Regul Integr Comp Physiol. 2012; 303:R495–504.36. Takenaka T, Inoue T, Okada H, Ohno Y, Miyazaki T, Chaston DJ, et al. Altered gap junctional communication and renal haemodynamics in Zucker fatty rat model of type 2 diabetes. Diabetologia. 2011; 54:2192–201.37. Thomas MC, Moran J, Forsblom C, Harjutsalo V, Thorn L, Ahola A, et al. The association between dietary sodium intake, ESRD, and all-cause mortality in patients with type 1 diabetes. Diabetes Care. 2011; 34:861–6.38. Sakabe K, Fukui M, Ushigome E, Hamaguchi M, Senmaru T, Yamazaki M, et al. Low daily salt intake is correlated with albuminuria in patients with type 2 diabetes. Hypertens Res. 2012; 35:1176–9.39. Chen SJ, Lv LL, Liu BC, Tang RN. Crosstalk between tubular epithelial cells and glomerular endothelial cells in diabetic kidney disease. Cell Prolif. 2020; 53:e12763.40. Wright EM. SGLT2 inhibitors: physiology and pharmacology. Kidney360. 2021; 2:2027–37.41. Salvatore T, Galiero R, Caturano A, Rinaldi L, Di Martino A, Albanese G, et al. An overview of the cardiorenal protective mechanisms of SGLT2 inhibitors. Int J Mol Sci. 2022; 23:3651.42. Wang XX, Levi J, Luo Y, Myakala K, Herman-Edelstein M, Qiu L, et al. SGLT2 protein expression is increased in human diabetic nephropathy: SGLT2 protein inhibition decreases renal lipid accumulation, inflammation, and the development of nephropathy in diabetic mice. J Biol Chem. 2017; 292:5335–48.43. Rajasekeran H, Reich HN, Hladunewich MA, Cattran D, Lovshin JA, Lytvyn Y, et al. Dapagliflozin in focal segmental glomerulosclerosis: a combined human-rodent pilot study. Am J Physiol Renal Physiol. 2018; 314:F412–22.44. Wheeler DC, Jongs N, Stefansson BV, Chertow GM, Greene T, Hou FF, et al. Safety and efficacy of dapagliflozin in patients with focal segmental glomerulosclerosis: a prespecified analysis of the dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial. Nephrol Dial Transplant. 2022; 37:1647–56.45. Bailey CJ, Day C, Bellary S. Renal protection with SGLT2 inhibitors: effects in acute and chronic kidney disease. Curr Diab Rep. 2022; 22:39–52.46. Cherney DZ, Perkins BA, Soleymanlou N, Maione M, Lai V, Lee A, et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014; 129:587–97.47. Rajasekeran H, Lytvyn Y, Bozovic A, Lovshin JA, Diamandis E, Cattran D, et al. Urinary adenosine excretion in type 1 diabetes. Am J Physiol Renal Physiol. 2017; 313:F184–91.48. Palmer BF, Clegg DJ. Kidney-protective effects of SGLT2 inhibitors. Clin J Am Soc Nephrol. 2023; 18:279–89.49. Sen T, Heerspink HJL. A kidney perspective on the mechanism of action of sodium glucose co-transporter 2 inhibitors. Cell Metab. 2021; 33:732–9.50. van Bommel EJ, Lytvyn Y, Perkins BA, Soleymanlou N, Fagan NM, Koitka-Weber A, et al. Renal hemodynamic effects of sodium-glucose cotransporter 2 inhibitors in hyperfiltering people with type 1 diabetes and people with type 2 diabetes and normal kidney function. Kidney Int. 2020; 97:631–5.51. van Bommel EJ, Muskiet MH, van Baar MJ, Tonneijck L, Smits MM, Emanuel AL, et al. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than pre-glomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 2020; 97:202–12.52. Nespoux J, Vallon V. Renal effects of SGLT2 inhibitors: an update. Curr Opin Nephrol Hypertens. 2020; 29:190–8.53. Vallon V, Muhlbauer B, Osswald H. Adenosine and kidney function. Physiol Rev. 2006; 86:901–40.54. Weihprecht H, Lorenz JN, Briggs JP, Schnermann J. Vasomotor effects of purinergic agonists in isolated rabbit afferent arterioles. Am J Physiol. 1992; 263(6 Pt 2):F1026–33.55. Nishiyama A, Inscho EW, Navar LG. Interactions of adenosine A1 and A2a receptors on renal microvascular reactivity. Am J Physiol Renal Physiol. 2001; 280:F406–14.56. Pak ES, Cha JJ, Cha DR, Kanasaki K, Ha H. Adenosine receptors as emerging therapeutic targets for diabetic kidney disease. Kidney Res Clin Pract. 2022; 41(Suppl 2):S74–88.57. Bell TD, Welch WJ. Regulation of renal arteriolar tone by adenosine: novel role for type 2 receptors. Kidney Int. 2009; 75:769–71.58. Pflueger AC, Schenk F, Osswald H. Increased sensitivity of the renal vasculature to adenosine in streptozotocin-induced diabetes mellitus rats. Am J Physiol. 1995; 269(4 Pt 2):F529–35.59. Heise T, Seewaldt-Becker E, Macha S, Hantel S, Pinnetti S, Seman L, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics following 4 weeks’ treatment with empagliflozin once daily in patients with type 2 diabetes. Diabetes Obes Metab. 2013; 15:613–21.60. Tanaka H, Takano K, Iijima H, Kubo H, Maruyama N, Hashimoto T, et al. Factors affecting canagliflozin-induced transient urine volume increase in patients with type 2 diabetes mellitus. Adv Ther. 2017; 34:436–51.61. Ichihara A, Navar LG. Neuronal NOS contributes to biphasic autoregulatory response during enhanced TGF activity. Am J Physiol. 1999; 277:F113–20.62. Huang X, Dorhout Mees E, Vos P, Hamza S, Braam B. Everything we always wanted to know about furosemide but were afraid to ask. Am J Physiol Renal Physiol. 2016; 310:F958–71.63. Jo W, Koh ES, Chung S. Therapeutic roles of thiazides and loop diuretics in blood pressure control and renal protection against chronic kidney disease. Clin Hypertens. 2023; 29:14.64. Thomson SC, Rieg T, Miracle C, Mansoury H, Whaley J, Vallon V, et al. Acute and chronic effects of SGLT2 blockade on glomerular and tubular function in the early diabetic rat. Am J Physiol Regul Integr Comp Physiol. 2012; 302:R75–83.65. Chen L, LaRocque LM, Efe O, Wang J, Sands JM, Klein JD. Effect of dapagliflozin treatment on fluid and electrolyte balance in diabetic rats. Am J Med Sci. 2016; 352:517–23.66. Chung S, Kim S, Son M, Kim M, Koh ES, Shin SJ, et al. Empagliflozin contributes to polyuria via regulation of sodium transporters and water channels in diabetic rat kidneys. Front Physiol. 2019; 10:271.67. Zhang J, Cai J, Cui Y, Jiang S, Wei J, Kim YC, et al. Role of the macula densa sodium glucose cotransporter type 1-neuronal nitric oxide synthase-tubuloglomerular feedback pathway in diabetic hyperfiltration. Kidney Int. 2022; 101:541–50.68. Ghezzi C, Loo DDF, Wright EM. Physiology of renal glucose handling via SGLT1, SGLT2 and GLUT2. Diabetologia. 2018; 61:2087–97.69. Skrabic R, Kumric M, Vrdoljak J, Rusic D, Skrabic I, Vilovic M, et al. SGLT2 inhibitors in chronic kidney disease: from mechanisms to clinical practice. Biomedicines. 2022; 10:2458.70. Wilcox CS. Antihypertensive and renal mechanisms of SGLT2 (sodium-glucose linked transporter 2) inhibitors. Hypertension. 2020; 75:894–901.71. Oh YK, Joo KW, Lee JW, Jeon US, Lim CS, Han JS, et al. Altered renal sodium transporter expression in an animal model of type 2 diabetes mellitus. J Korean Med Sci. 2007; 22:1034–41.72. Spires D, Manis AD, Staruschenko A. Ion channels and transporters in diabetic kidney disease. Curr Top Membr. 2019; 83:353–96.73. Eriguchi M, Bernstein EA, Veiras LC, Khan Z, Cao DY, Fuchs S, et al. The absence of the ACE N-domain decreases renal inflammation and facilitates sodium excretion during diabetic kidney disease. J Am Soc Nephrol. 2018; 29:2546–61.74. Gamba G. Regulation of the renal Na+-Cl- cotransporter by phosphorylation and ubiquitylation. Am J Physiol Renal Physiol. 2012; 303:F1573–83.75. Chavez-Canales M, Arroyo JP, Ko B, Vazquez N, Bautista R, Castaneda-Bueno M, et al. Insulin increases the functional activity of the renal NaCl cotransporter. J Hypertens. 2013; 31:303–11.76. Yuan T, Jiang L, Chen C, Peng X, Nie M, Li X, et al. Glucose tolerance and insulin responsiveness in Gitelman syndrome patients. Endocr Connect. 2017; 6:243–52.77. De la Cruz-Cano E, Jimenez-Gonzalez CD, Morales-Garcia V, Pineda-Perez C, Tejas-Juarez JG, Rendon-Gandarilla FJ, et al. Arg913Gln variation of SLC12A3 gene is associated with diabetic nephropathy in type 2 diabetes and Gitelman syndrome: a systematic review. BMC Nephrol. 2019; 20:393.78. Andersen H, Friis UG, Hansen PB, Svenningsen P, Henriksen JE, Jensen BL. Diabetic nephropathy is associated with increased urine excretion of proteases plasmin, prostasin and urokinase and activation of amiloride-sensitive current in collecting duct cells. Nephrol Dial Transplant. 2015; 30:781–9.79. Hills CE, Bland R, Bennett J, Ronco PM, Squires PE. High glucose up-regulates ENaC and SGK1 expression in HCD-cells. Cell Physiol Biochem. 2006; 18:337–46.80. Blass G, Klemens CA, Brands MW, Palygin O, Staruschenko A. Postprandial effects on ENaC-mediated sodium absorption. Sci Rep. 2019; 9:4296.81. Pearce D, Soundararajan R, Trimpert C, Kashlan OB, Deen PM, Kohan DE. Collecting duct principal cell transport processes and their regulation. Clin J Am Soc Nephrol. 2015; 10:135–46.82. Ishizawa K, Wang Q, Li J, Xu N, Nemoto Y, Morimoto C, et al. Inhibition of sodium glucose cotransporter 2 attenuates the dysregulation of Kelch-Like 3 and NaCl cotransporter in obese diabetic mice. J Am Soc Nephrol. 2019; 30:782–94.83. Sheetz MJ, King GL. Molecular understanding of hyperglycemia’s adverse effects for diabetic complications. JAMA. 2002; 288:2579–88.84. Meor Azlan NF, Koeners MP, Zhang J. Regulatory control of the Na-Cl co-transporter NCC and its therapeutic potential for hypertension. Acta Pharm Sin B. 2021; 11:1117–28.85. Ma C, de Baaij JH, Millar PJ, Gault VA, de Galan BE, Bindels RJ, et al. Effect of dapagliflozin treatment on the expression of renal sodium transporters/channels on high-fat diet diabetic mice. Nephron. 2019; 142:51–60.86. Ray EC, Pitzer A, Lam T, Jordahl A, Patel R, Ao M, et al. Salt sensitivity of volume and blood pressure in a mouse with globally reduced ENaC γ-subunit expression. Am J Physiol Renal Physiol. 2021; 321:F705–14.87. Salih M, Gautschi I, van Bemmelen MX, Di Benedetto M, Brooks AS, Lugtenberg D, et al. A missense mutation in the extracellular domain of αENaC causes liddle syndrome. J Am Soc Nephrol. 2017; 28:3291–9.88. Konstas AA, Korbmacher C. The gamma-subunit of ENaC is more important for channel surface expression than the beta-subunit. Am J Physiol Cell Physiol. 2003; 284:C447–56.89. Refardt J, Imber C, Sailer CO, Jeanloz N, Potasso L, Kutz A, et al. A randomized trial of empagliflozin to increase plasma sodium levels in patients with the syndrome of inappropriate antidiuresis. J Am Soc Nephrol. 2020; 31:615–24.90. Refardt J, Imber C, Nobbenhuis R, Sailer CO, Haslbauer A, Monnerat S, et al. Treatment effect of the SGLT2 inhibitor empagliflozin on chronic syndrome of inappropriate antidiuresis: results of a randomized, double-blind, placebo-controlled, crossover trial. J Am Soc Nephrol. 2023; 34:322–32.91. Monnerat S, Atila C, Refardt J, Christ-Crain M. Prevalence of admission hyponatremia in patients with diabetes treated with and without an SGLT2 inhibitor. J Endocr Soc. 2023; 7:bvad011.92. Sarafidis P, Loutradis C, Ferro CJ, Ortiz A. SGLT-2 inhibitors to treat hyponatremia associated with SIADH: a novel indication? Am J Nephrol. 2020; 51:553–5.93. Masuda T, Muto S, Fukuda K, Watanabe M, Ohara K, Koepsell H, et al. Osmotic diuresis by SGLT2 inhibition stimulates vasopressin-induced water reabsorption to maintain body fluid volume. Physiol Rep. 2020; 8:e14360.94. Lee JF, Berzan E, Sridhar VS, Odutayo A, Cherney DZI. Cardiorenal protection in diabetic kidney disease. Endocrinol Metab (Seoul). 2021; 36:256–69.95. Chan AT, Tang SC. Advances in the management of diabetic kidney disease: beyond sodium-glucose co-transporter 2 inhibitors. Kidney Res Clin Pract. 2022; 41:682–98.96. Pitt B, Bhatt DL. Does SGLT1 inhibition add benefit to SGLT2 inhibition in type 2 diabetes? Circulation. 2021; 144:4–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Potential Cardioprotective Mechanism of Sodium-Glucose Cotransporter 2 Inhibitors
- The Non-glycemic Effects of SGLT2 Inhibitor
- Sodium-Glucose Cotransporter 2 Inhibitors for Chronic Kidney Disease: A Comprehensive Review
- SGLT2 Inhibition for Diabetic and Non-diabetic Kidney Disease
- Renoprotective Mechanism of Sodium-Glucose Cotransporter 2 Inhibitors: Focusing on Renal Hemodynamics
