Injury to the Left Sciatic and Right Common Peroneal Nerves Combined With Multifocal Rhabdomyolysis in a Survivor of the Itaewon Crowd Crush: A Case Report
- Affiliations
-
- 1Department of Physical & Rehabilitation Medicine, Chung-Ang University College of Medicine, Seoul, Korea
- KMID: 2544947
- DOI: http://doi.org/10.3346/jkms.2023.38.e233
Abstract
- We report the case of a 27-year-old survivor of the Halloween crowd crush in Itaewon, Seoul, Korea who was diagnosed with left sciatic neuropathy and right common peroneal neuropathy accompanied by multifocal rhabdomyolysis. The patient presented to the emergency room complaining of pain from her lower back to her whole lower extremities with paraparesis and paresthesia. Her blood test showed the marked elevation of creatine kinase and liver enzymes. Magnetic resonance imaging revealed multifocal signal changes in the abdominalis and pelvic girdle muscles suggestive of rhabdomyolysis. Magnetic resonance neurography demonstrated injury to the left sciatic and right peroneal nerves. Electrophysiologic studies also revealed lesions in the left sciatic and right peroneal nerves. After comprehensive rehabilitation and conservative treatment for three months, her muscle strength improved, and she could walk independently. Although several previous studies have reported peripheral neuropathy in immobilized patients, to the best of our knowledge, no case associated with a crowd crush has been reported. Therefore, we report the case of multifocal neuropathy combined with rhabdomyolysis in a victim of a crowd crush incident with good recovery.
Figure
-
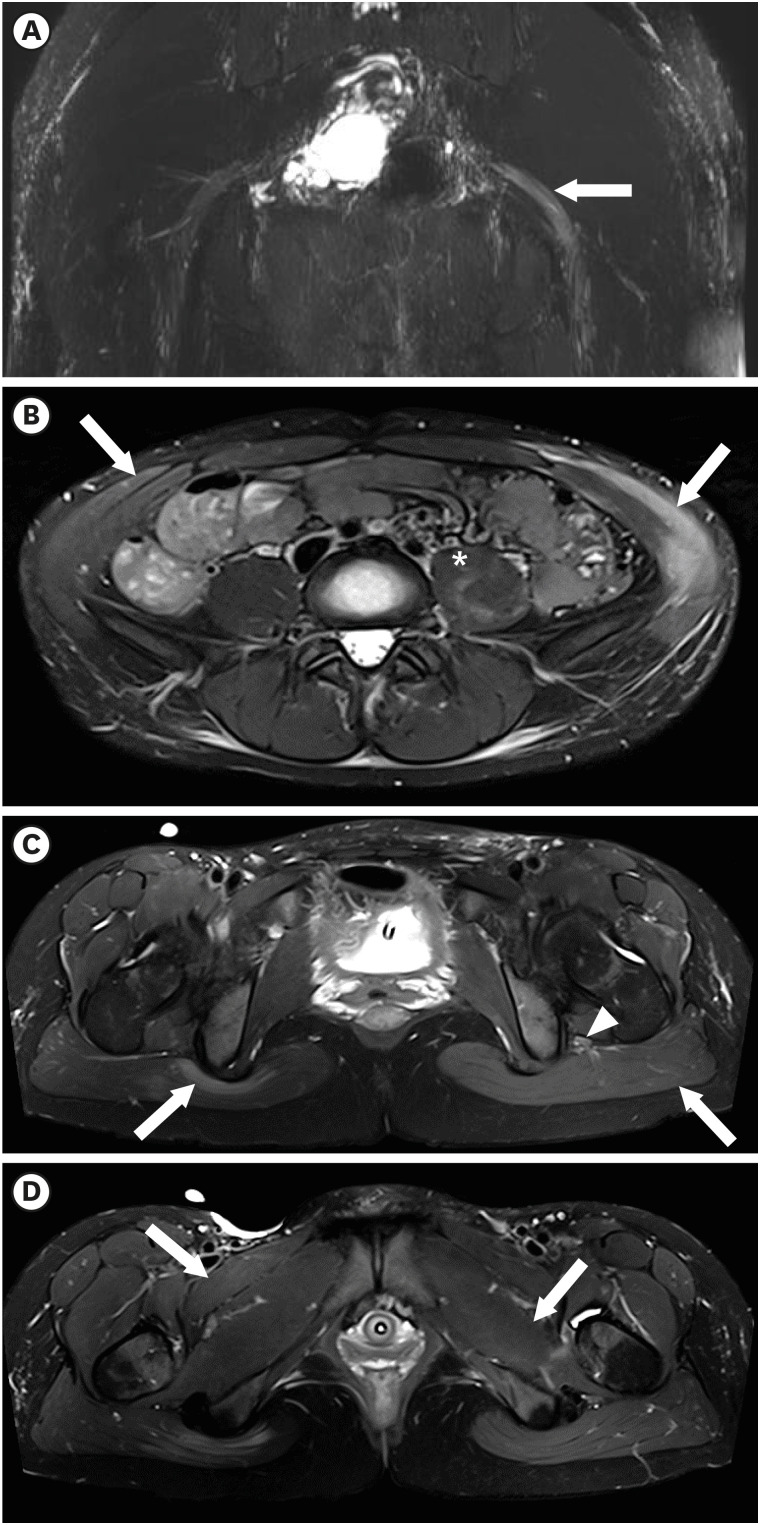
Fig. 1 Magnetic resonance imaging of the pelvis. (A) Swelling of the left sciatic nerve (white arrow) from the sciatic foramen to the proximal thigh compared with the right sciatic nerve on an maximum intensity projection image from a coronal reconstructed three-dimensional-short tau inversion recovery sampling perfection with application optimized contrasts with variable flip-angle image. (B) Increased signal intensity in the bilateral external/internal oblique abdominis (white arrow) and left psoas muscle (asterisk) on an axial T2-weighted image with TSE fat suppression. (C) Diffuse swelling of the left sciatic nerve (white arrowhead) surrounded by diffuse edema and high signal change in the left gluteal muscle (white arrow) compared with only a focal signal change near the ischial tuberosity of the right gluteal muscle (white arrow) on an axial T2-weighted slice with TSE fat suppression. (D) Increased signal intensity in the right pectineus (white arrow) and left quadratus femoris muscles (white arrow).TSE = turbo spin echo.
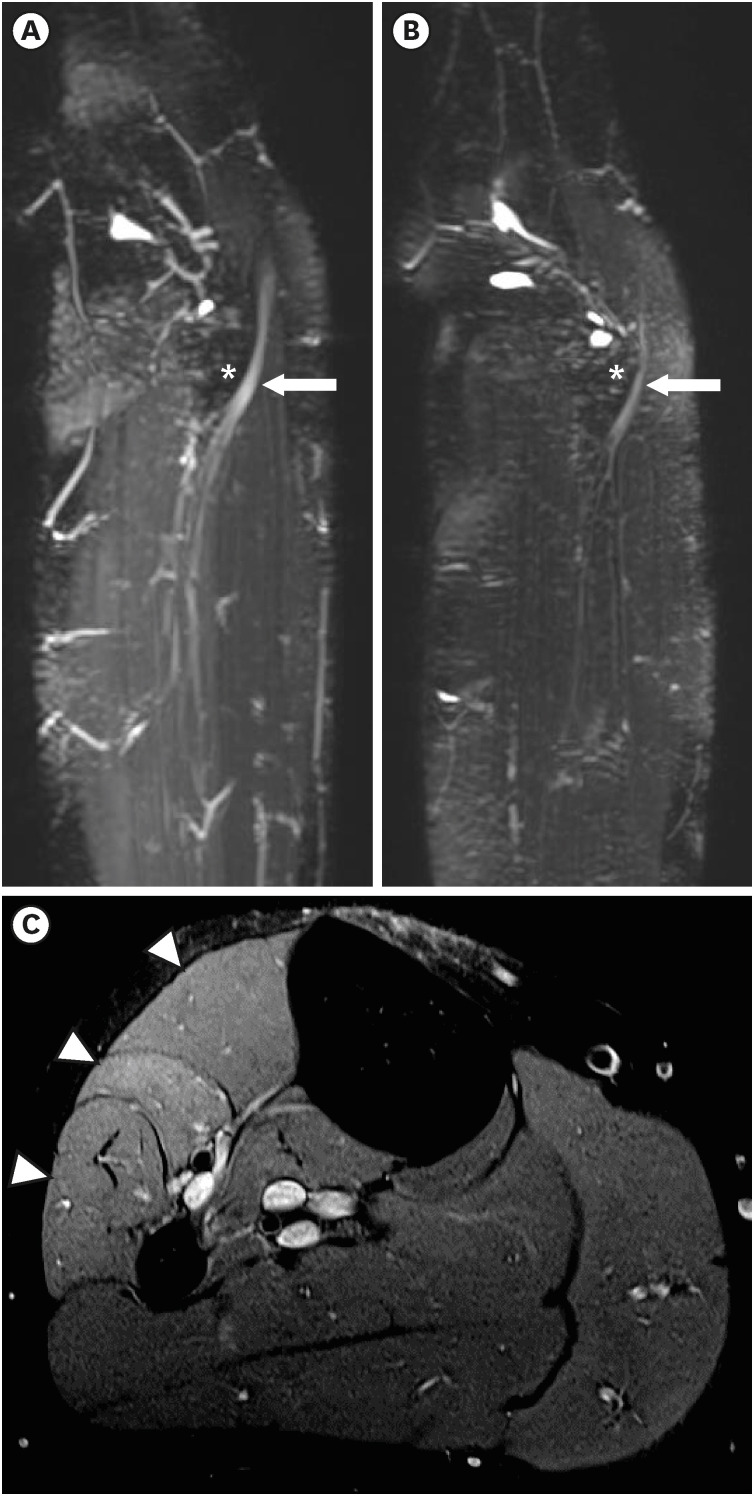
Fig. 2 Magnetic resonance imaging of the knee. (A, B) Swelling with enhancement of the right common peroneal nerve (A, white arrow), which winds around the lateral aspect of the fibular head (asterisk), compared with the left common peroneal nerve (B, white arrow) on an maximum intensity projection image from a coronal-reconstructed three-dimensional short tau inversion recovery sampling perfection with application optimized contrasts with variable flip-angle evolutions image. (C) Ill-defined hyper signal intensity changes in right peroneal-innervated muscles (tibialis anterior, extensor digitorum longus, and peroneal longus) (white arrow heads) compared with no signal change in tibial-innervated muscles on the proton density axial turbo spin echo fat-suppression magnetic resonance image.
Cited by 1 articles
-
Letter to the Editor: Nerve Entrapment From a Crush Injury During the Halloween Mass Casualty Accident in Itaewon
Josef Finsterer
J Korean Med Sci. 2023;38(36):e307. doi: 10.3346/jkms.2023.38.e307.
Reference
-
1. Yuen EC, So YT, Olney RK. The electrophysiologic features of sciatic neuropathy in 100 patients. Muscle Nerve. 1995; 18(4):414–420. PMID: 7715627.2. Yuen EC, So YT. Sciatic neuropathy. Neurol Clin. 1999; 17(3):617–631. PMID: 10393756.3. Lee SS, Lee SH, Lee YS, Song MJ. Two unusual cases of sciatic neuropathy. Ann Clin Neurophysiol. 2005; 7(1):55–57.4. Distad BJ, Weiss MD. Clinical and electrodiagnostic features of sciatic neuropathies. Phys Med Rehabil Clin N Am. 2013; 24(1):107–120. PMID: 23177034.5. Cho JY, Moon H, Park S, Lee BJ, Park D. Isolated injury to the tibial division of sciatic nerve after self-massage of the gluteal muscle with massage ball: a case report. Medicine (Baltimore). 2019; 98(19):e15488. PMID: 31083184.6. Kim IS, Lee WH, Lim JY. Multiple peripheral neuropathies adjacent to necrotizing myositis related to rhabdomyolysis. Ann Geriatr Med Res. 2017; 21(1):31–34.7. Lee SA, Lim JY. Bilateral sciatic neuropathy associated with rhabdomyolysis in an immobilized patient: a case report. J Korean Acad Rehabil Med. 2009; 33(1):127–130.8. Seok JI, Lee IH, Ahn KS, Kang GW, Kim JH. Peripheral neuropathies in patients with rhabdomyolysis: clinical characteristics and electrodiagnostic findings in the acute/subacute stage. J Korean Neurol Assoc. 2019; 37(1):26–29.9. Lee HD, Lee SY, Cho YS, Han SH, Park SB, Lee KH. Sciatic neuropathy and rhabdomyolysis after carbon monoxide intoxication: a case report. Medicine (Baltimore). 2018; 97(23):e11051. PMID: 29879074.10. Bowley MP, Doughty CT. Entrapment neuropathies of the lower extremity. Med Clin North Am. 2019; 103(2):371–382. PMID: 30704688.11. Lee RS, Hughes RL. Prediction of human crowd pressures. Accid Anal Prev. 2006; 38(4):712–722. PMID: 16487473.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Crush Syndrome: Traumatic Rhabdomyolysis, Reperfusion Injury
- Effect of Partial Sciatic Nerve Injury on the Response to Formalin Test in Rats
- Sciatic neurotmesis and periostitis ossificans progressiva due to a traumatic/unexpected glass injury: a case report
- Sciatic Nerve Palsy Complicating Gluteal Compartment Syndrome due to Rhabdomyolysis: A Case Report
- Combined Femoral and Sciatic Nerve Palsy Associated with Acetabular Fracture and Dislocation: A Case Report
