Five-year Progress of Gastric MALT Lymphoma Presenting as Gastric Outlet Obstruction
- Affiliations
-
- 1Departments of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Departments of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2543447
- DOI: http://doi.org/10.4166/kjg.2023.026
Abstract
- This paper reports a 70-year-old female with gastric extranodal marginal zone B cell lymphoma of mucosa-associated lymphoid tissue (gastric MALT lymphoma) as a rare case of gastric outlet obstruction. Five years earlier, she initially presented with weight loss and anemia. Esophagogastroduodenoscopy (EGD) revealed multiple gastric and duodenal ulcers with a pyloric deformity, while histology revealed chronic active inflammation and a Helicobacter pylori (H. pylori) infection. Three years earlier, she underwent EGD per the National Cancer Screening Program and was diagnosed with antral and duodenal ulcers. A forceps biopsy specimen from one of the ulcers showed the findings of gastric MALT lymphoma, but she did not visit the hospital for proper management. She visited complaining of a loss of appetite. EGD revealed a gastric outlet obstruction (GOO) caused by antral deformity and pyloric narrowing. A staged workup with CT and PET revealed full-layered, encircling antral wall thickening and several enlarged mesenteric lymph nodes. She was finally diagnosed with a gastric MALT lymphoma at Ann Arbor stage I1E with translocation t(11;18). She was treated with palliative surgery for GOO and systemic chemotherapy with a CHOP regimen. This paper reports a gastric MALT lymphoma that progressed from superficial mucosal lesions to an overt mass with regional lymph node metastasis for five years. (Korean J Gastroenterol 2023;81:265 -269)
Keyword
Figure
-

Fig. 1 EGD findings on each patient’s visit. (A) Multiple gastric and duodenal ulcers with pyloric deformity. (B) Several gastric ulcers at the antrum and lower body, and duodenal ulcers at various stages. Histology of one ulcer (indicated) confirmed as marginal zone MALT lymphoma. (C) Pylorus deformity and luminal narrowing due to mass forming effect of geographic and speculated ulcers. EGD, esophagogastroduodenoscopy; MALT, mucosa-associated lymphoid tissue.

Fig. 2 CT scan of the abdomen, coronal plane. Poorly enhancing encircling mass in stomach antrum with ulceroinfiltrative feature corresponds to gastric outlet obstruction due to advanced malignancy.

Fig. 3 PET scan. PET scan showed a full-layered encircling wall thickening with FDG-avid high in the antrum and several enlarged mesenteric lymph nodes, suggesting a gastric malignancy.
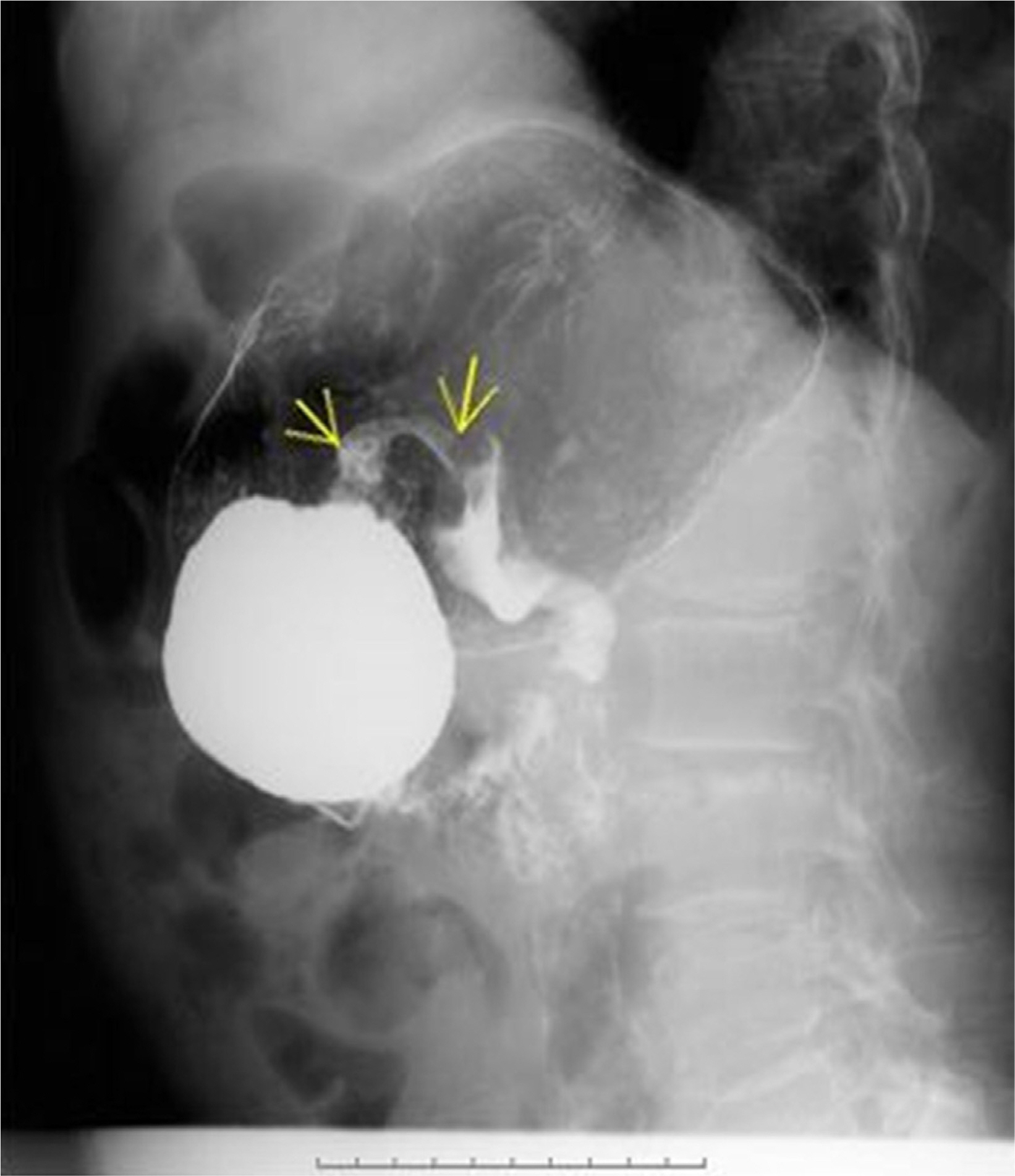
Fig. 4 Hypotonic duodenography. Duodenography under antispasmodic agent showed pyloric narrowing with slow contrast passage. Arrows: narrowed pyloric canal.
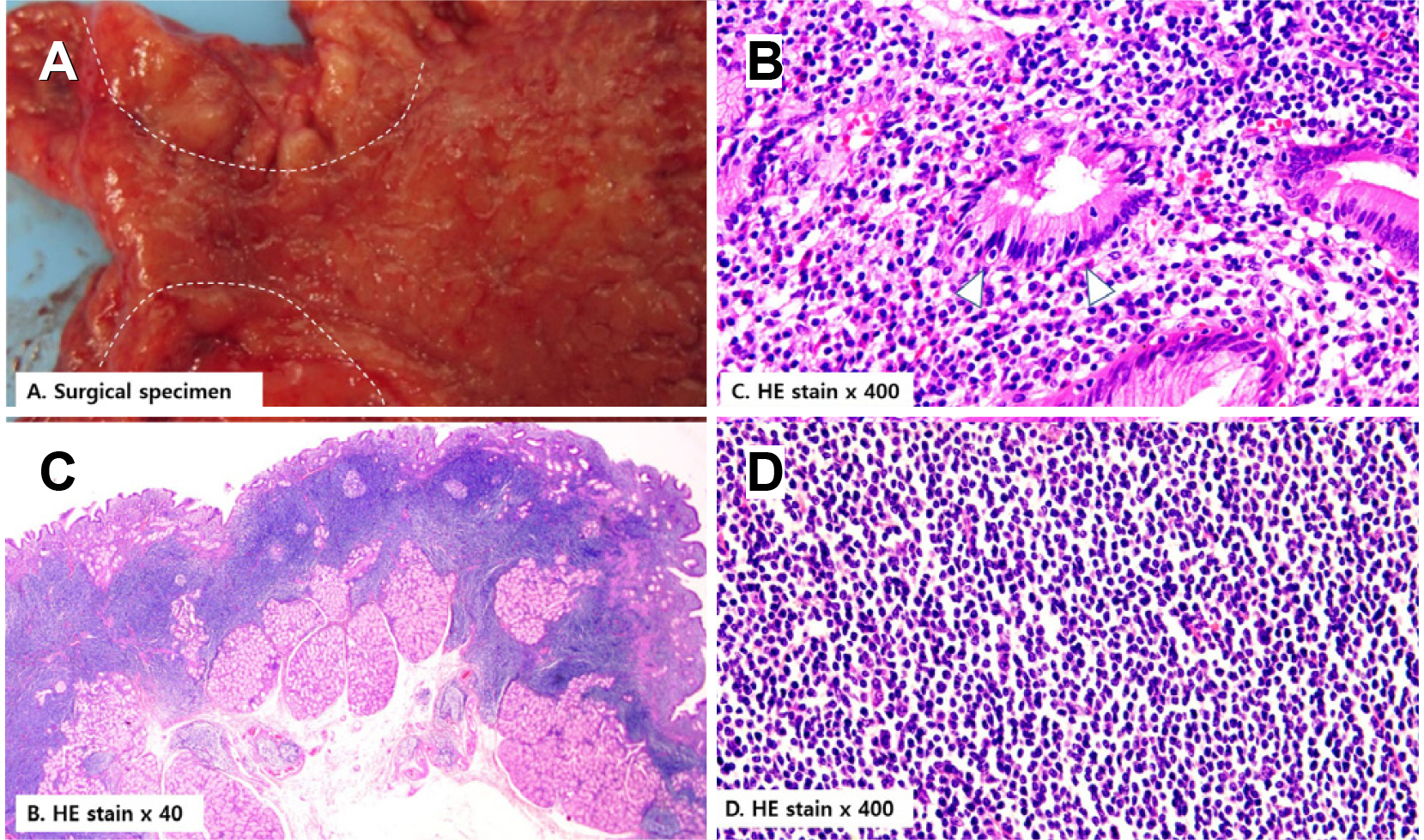
Fig. 5 Gross finding of surgical specimen and microscopic examination of H&E staining. (A) The wall of the pylorus (white dotted line) and antrum showed diffuse thickening with the irregularly nodular and ulcerative mucosal surface. (B) Microscopic image (H&E stained ×400) showed lymphoepithelial lesions in the glandular epithelium (C, white arrowheads). (C) Macroscopic image (H&E stained ×40) showed diffuse and monotonous small lymphoid cell infiltration formed tumor mass. (D) Microscopic image (H&E stained ×400) showed densely stained monotonous small lymphoid cell infiltration into the submucosal layer.
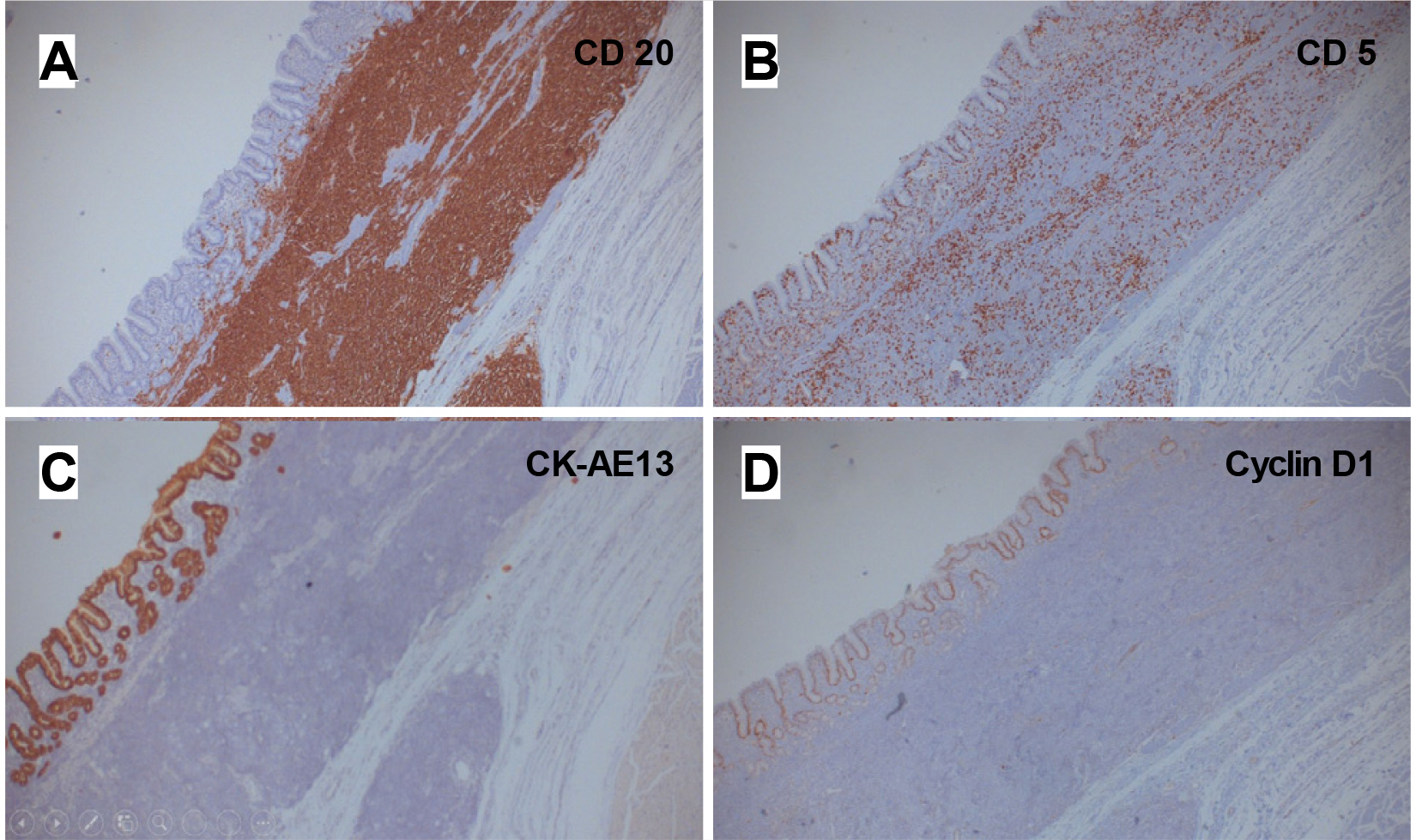
Fig. 6 Immunochemical staining. (A) Tumor cells were stained positive with CD20. (B) Tumor cells were stained scanty with CD5. (C) CK AE1/3 was positive and suggestive of the presence of a lymphoepithelial lesion. (D) Tumor cells were stained negative for cyclin D.
Reference
-
1. Isaacson P, Wright DH. 1983; Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma. Cancer. 52:1410–1416. DOI: 10.1002/1097-0142(19831015)52:8<1410::aid-cncr2820520813>3.0.co;2-3. PMID: 6193858.
Article2. Wang YG, Zhao LY, Liu CQ, et al. 2016; Clinical characteristics and prognostic factors of primary gastric lymphoma: A retrospective study with 165 cases. Medicine (Baltimore). 95:e4250. DOI: 10.1097/MD.0000000000004250. PMID: 27495029. PMCID: PMC4979783.3. Zaki M, Schubert ML. 1995; Helicobacter pylori and gastric lymphoma. Gastroenterology. 108:610–612. DOI: 10.1016/0016-5085(95)90098-5.
Article4. Park HS, Kim YJ, Yang WI, Suh CO, Lee YC. 2010; Treatment outcome of localized Helicobacter pylori-negative low-grade gastric MALT lymphoma. World J Gastroenterol. 16:2158–2562. DOI: 10.3748/wjg.v16.i17.2158. PMID: 20440857. PMCID: PMC2864842.
Article5. Zullo A, Hassan C, Cristofari F, et al. 2010; Effects of Helicobacter pylori eradication on early stage gastric mucosa-associated lymphoid tissue lymphoma. Clin Gastroenterol Hepatol. 8:105–110. DOI: 10.1016/j.cgh.2009.07.017. PMID: 19631287.
Article6. Kim JS, Park JC, Lee JY, et al. 2021; Long-term clinical outcomes of gastric MALT lymphoma: A nationwide multicenter study in Korea. Front Oncol. 11:681689. DOI: 10.3389/fonc.2021.681689. PMID: 34722238. PMCID: PMC8551628.
Article7. Malfertheiner P, Megraud F, O'Morain C, et al. 2007; Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 56:772–781. DOI: 10.1136/gut.2006.101634. PMID: 17170018. PMCID: PMC1954853.
Article8. Nakamura S, Hojo M. 2022; Diagnosis and treatment for gastric mucosa-associated lymphoid tissue (MALT) lymphoma. J Clin Med. 12:120. DOI: 10.3390/jcm12010120. PMID: 36614921. PMCID: PMC9820981.
Article9. Moleiro J, Ferreira S, Lage P, Dias Pereira A. 2016; Gastric malt lymphoma: Analysis of a series of consecutive patients over 20 years. United European Gastroenterol J. 4:395–402. DOI: 10.1177/2050640615612934. PMID: 27403306. PMCID: PMC4924435.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Helicobacter pylori-negative Gastric Mucosa-associated Lymphoid Tissue Lymphoma
- Role of Chemotherapy in Gastric Marginal Zone B-Cell Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT) Type
- A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
- Gastrointestinal Lymphoma
- Endoscopic Diagnosis of Gastric MALT Lymphoma
