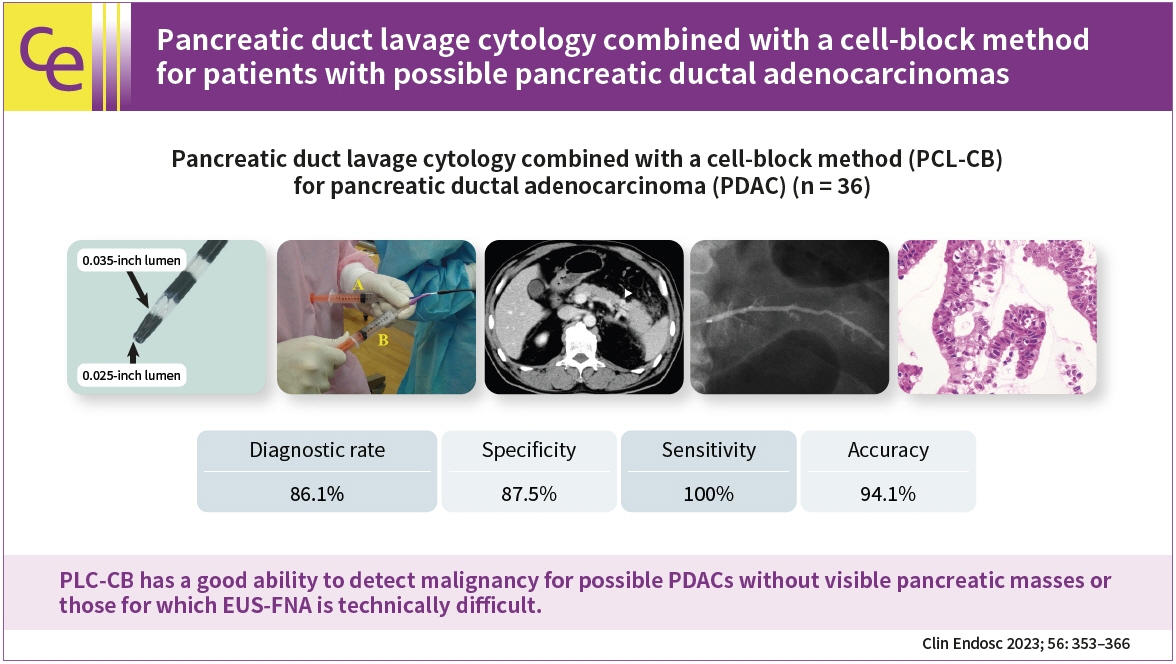
Pancreatic duct lavage cytology combined with a cell-block method for patients with possible pancreatic ductal adenocarcinomas, including pancreatic carcinoma in situ
- Kusunose H
 1
1 - Koshita S1
- Kanno Y1
- Ogawa T1
- Sakai T1
- Yonamine K1
- Miyamoto K1
- Kozakai F1
- Anan H1
- Endo K1,4
- Okano H1
- Oikawa M2
- Tsuchiya T2
- Sawai T3
- Noda Y1,3
- Ito K1
- Affiliations
-
- 1Department of Gastroenterology, Sendai City Medical Center, Sendai, Japan
- 2Department of Surgery, Sendai City Medical Center, Sendai, Japan
- 3Department of Pathology, Sendai City Medical Center, Sendai, Japan
- 4Department of Gastroenterology, Yokohama City University Medical Center, Yokohama, Japan
- KMID: 2542463
- DOI: http://doi.org/10.5946/ce.2022.021
Abstract
- Background/Aims
This study aimed to clarify the efficacy and safety of pancreatic duct lavage cytology combined with a cell-block method (PLC-CB) for possible pancreatic ductal adenocarcinomas (PDACs).
Methods
This study included 41 patients with suspected PDACs who underwent PLC-CB mainly because they were unfit for undergoing endoscopic ultrasonography-guided fine needle aspiration. A 6-Fr double lumen catheter was mainly used to perform PLC-CB. Final diagnoses were obtained from the findings of resected specimens or clinical outcomes during surveillance after PLC-CB.
Results
Histocytological evaluations using PLC-CB were performed in 87.8% (36/41) of the patients. For 31 of the 36 patients, final diagnoses (invasive PDAC, 12; pancreatic carcinoma in situ, 5; benignancy, 14) were made, and the remaining five patients were excluded due to lack of surveillance periods after PLC-CB. For 31 patients, the sensitivity, specificity, and accuracy of PLC-CB for detecting malignancy were 94.1%, 100%, and 96.8%, respectively. In addition, they were 87.5%, 100%, and 94.1%, respectively, in 17 patients without pancreatic masses detectable using endoscopic ultrasonography. Four patients developed postprocedural pancreatitis, which improved with conservative therapy.
Conclusions
PLC-CB has an excellent ability to detect malignancies in patients with possible PDACs, including pancreatic carcinoma in situ.
Keyword
Figure
-
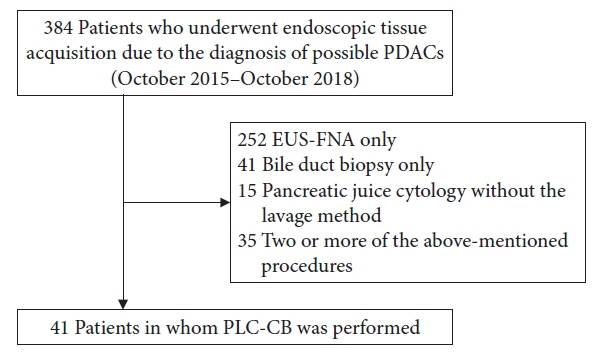
Fig. 1. Flowchart for patient selection in this study. PDACs, pancreatic ductal adenocarcinomas; EUS-FNA, endoscopic ultrasound-guided fine needle aspiration; PLC-CB, pancreatic duct lavage cytology combined with a cell-block method.

Fig. 2. Tip of a double lumen sampling catheter used in this study (Uneven Double Lumen Cannula; Piolax Medical Devices Inc.).

Fig. 3. Endoscopic procedure for pancreatic duct lavage cytology by using a double lumen catheter (endoscopy assistant). The injection of saline into the main pancreatic duct (A) and the suction of fluid in the main pancreatic duct with negative pressure by using a syringe (B) were simultaneously performed through two separate lumens (0.025- and 0.035-inch lumen, respectively).

Fig. 4. A 64-year-old patient with an initial diagnosis of acute pancreatitis (patient no. 14 in Table 2). The enlargement of the pancreatic tail with mild pancreatitis and localized atrophy of the pancreatic parenchyma at the proximal site of the enlarged pancreatic tail were detected (A, contrast-enhanced computed tomography, arrowhead). Endoscopic ultrasonography did not detect mass lesions, and magnetic resonance cholangiopancreatography did not show the main pancreatic duct stenosis at the pancreatic tail. We suspected pancreatic carcinoma in situ and performed pancreatic duct lavage cytology combined with a cell-block method using a double lumen catheter. Endoscopic retrograde pancreatography did not show clear stenosis of the main pancreatic duct at the pancreatic tail (B, pancreatography). Cell-block specimens obtained were firstly evaluated by using hematoxylin and eosin staining (C, ×10; D, ×40). Histocytological diagnosis was shown to be adenocarcinoma (Class V), and distal pancreatectomy was performed. For the histological findings of resected specimens, the atypical ductal epithelium was continuously observed from the main pancreatic duct (E, ×20; arrowhead) to branch pancreatic duct, and invasive components derived from this atypical epithelium were not found. Thus, this patient was diagnosed with pancreatic carcinoma in situ (high-grade pancreatic intraepithelial neoplasm).

Fig. 5. An 82-year-old patient (patient no. 17 in Table 2) with recurrent acute pancreatitis had a localized parenchymal atrophy of the pancreatic body (A, contrast-enhanced computed tomography; arrowhead, localized atrophic parenchyma in the pancreatic body). Although magnetic resonance cholangiopancreatography (B) showed a stenosis of the main pancreatic duct (MPD) in the pancreatic body (arrowhead), endoscopic ultrasonography did not detect mass lesions in this MPD stenosis. Pancreatic duct lavage cytology combined with a cell-block method using a double lumen catheter was conducted due to the diagnosis of suspected pancreatic carcinoma in situ. For histocytology of the specimens obtained through pancreatic duct lavage cytology combined with a cell-block method, some clusters of atypical cells were observed by using hematoxylin and eosin staining (C, ×20). MUC1 staining (D, ×40) was focally positive, a Ki-67 labeling index (E, ×40) was approximately 20% and p53 staining was negative, indicating adenocarcinoma (Class IV). She underwent distal pancreatectomy, and histology (hematoxylin and eosin staining) of resected specimens showed an atypical epithelium mainly located in the MPD and branch ducts (F, ×4; G, ×20; black arrowhead: MPD, yellow arrowhead: branch duct), resulting in the final diagnosis of pancreatic carcinoma in situ (high-grade pancreatic intraepithelial neoplasm).
Reference
-
1. ASGE Standards of Practice Committee, Eloubeidi MA, Decker GA, et al. The role of endoscopy in the evaluation and management of patients with solid pancreatic neoplasia. Gastrointest Endosc. 2016; 83:17–28.2. Renelus BD, Jamorabo DS, Boston I, et al. Endoscopic ultrasound-guided fine needle biopsy needles provide higher diagnostic yield compared to endoscopic ultrasound-guided fine needle aspiration needles when sampling solid pancreatic lesions: a meta-analysis. Clin Endosc. 2021; 54:261–268.3. Chung MJ, Park SW, Kim SH, et al. Clinical and technical guideline for endoscopic ultrasound (EUS)-guided tissue acquisition of pancreatic solid tumor: Korean Society of Gastrointestinal Endoscopy (KSGE). Clin Endosc. 2021; 54:161–181.4. Nakaizumi A, Tatsuta M, Uehara H, et al. Usefulness of simple endoscopic aspiration cytology of pancreatic juice for diagnosis of early pancreatic neoplasm: a prospective study. Dig Dis Sci. 1997; 42:1796–1803.5. Koshita S, Noda Y, Ito K, et al. Pancreatic juice cytology with immunohistochemistry to detect malignancy and histologic subtypes in patients with branch duct type intraductal papillary mucinous neoplasms of the pancreas. Gastrointest Endosc. 2017; 85:1036–1046.6. Noda Y, Fujita N, Kobayashi G, et al. Prospective randomized controlled study comparing cell block method and conventional smear method for pancreatic juice cytology. Dig Endosc. 2012; 24:168–174.7. Koshita S, Noda Y, Kanno Y, et al. Value of repeated cytology for intraductal papillary mucinous neoplasms of the pancreas with high risk potential of malignancy: is it a promising method for monitoring a malignant transformation? Pancreatology. 2020; 20:1164–1174.8. Sai JK, Nobukawa B, Matsumura Y, et al. Pancreatic duct lavage cytology with the cell block method for discriminating benign and malignant branch-duct type intraductal papillary mucinous neoplasms. Gastrointest Endosc. 2013; 77:726–735.9. Kanno Y, Koshita S, Ogawa T, et al. Predictive value of localized stenosis of the main pancreatic duct for early detection of pancreatic cancer. Clin Endosc. 2019; 52:588–597.10. Noda Y, Fujita N, Kobayashi G, et al. Diagnostic efficacy of the cell block method in comparison with smear cytology of tissue samples obtained by endoscopic ultrasound-guided fine-needle aspiration. J Gastroenterol. 2010; 45:868–875.11. Guidelines of the Papanicolaou Society of Cytopathology for fine-needle aspiration procedure and reporting. Diagn Cytopathol. 1997; 17:239–247.12. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991; 37:383–393.13. Iiboshi T, Hanada K, Fukuda T, et al. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas. 2012; 41:523–529.14. Satoh T, Kikuyama M, Kawaguchi S, et al. Acute pancreatitis-onset carcinoma in situ of the pancreas with focal fat replacement diagnosed using serial pancreatic-juice aspiration cytologic examination (SPACE). Clin J Gastroenterol. 2017; 10:541–545.15. Peters ML, Eckel A, Mueller PP, et al. Progression to pancreatic ductal adenocarcinoma from pancreatic intraepithelial neoplasia: results of a simulation model. Pancreatology. 2018; 18:928–934.16. Mikata R, Ishihara T, Tada M, et al. Clinical usefulness of repeated pancreatic juice cytology via endoscopic naso-pancreatic drainage tube in patients with pancreatic cancer. J Gastroenterol. 2013; 48:866–873.17. Mouri T, Sasaki T, Serikawa M, et al. A comparison of 4-Fr with 5-Fr endoscopic nasopancreatic drainage catheters: a randomized, controlled trial. J Gastroenterol Hepatol. 2016; 31:1783–1789.18. Ito K, Fujita N, Noda Y, et al. Can pancreatic duct stenting prevent post-ERCP pancreatitis in patients who undergo pancreatic duct guidewire placement for achieving selective biliary cannulation? A prospective randomized controlled trial. J Gastroenterol. 2010; 45:1183–1191.19. Dumonceau JM, Andriulli A, Elmunzer BJ, et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline - updated June 2014. Endoscopy. 2014; 46:799–815.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cell block created from pancreatic duct lavage is another jigsaw puzzle to diagnose early pancreatic ductal adenocarcinoma
- Pathological Classification of Panaeatic Cancer and Precancerous Casion
- Expression of S100A4 in Invasive Adenocarcinoma and Intraductal Papillary Mucinous Neoplasm of the Pancreas
- A Small Pancreatic Neuroendocrine Tumor with Marked Pancreatic Duct Dilatation and Parenchymal Atrophy
- A Case of Cutaneous Metastatic Adenosquamous Carcinoma of the Pancreas
