First aid with color atlas for the use of intestinal ultrasound for inflammatory bowel disease in daily clinical practice
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Mitaka, Japan
- KMID: 2541890
- DOI: http://doi.org/10.5217/ir.2023.00003
Abstract
- Intestinal ultrasound (IUS) is a promising modality for the management of inflammatory bowel disease (IBD) and has the potential to particularly contribute in monitoring disease activity, an advantage crucial for optimizing the therapeutic strategy. While many IBD physicians appreciate and are interested in the use of IUS for IBD, currently only a limited number of facilities can employ this examination in daily clinical practice. A lack of guidance is one of the major barriers to introducing this procedure. Standardized protocols and assessment criteria are needed such that IUS for IBD can be considered a feasible, reliable examination in clinical practice, and multicenter clinical studies can be conducted for further clinical evidence of the application of IUS in IBD for best patient care. In this article, we provide an overview of how to start IUS for IBD and introduce basic procedures. Furthermore, IUS images from our practice are provided as a color atlas for understanding sonographic findings and scoring systems. We anticipate this “first aid” article will be helpful to promote IUS for IBD in daily practice.
Figure
-

Fig. 1. Examination of the colon using transabdominal ultrasound. We start from the middle lower area to examine the rectum. The rectum cannot be sufficiently assessed with transabdominal ultrasound. Then, we trace the colon counterclockwise. In some cases, the transverse colon descends from the middle to the lower abdominal area.

Fig. 2. Sonographic images of the normal large and small bowel. (A) The overall B-mode image of the colon and small intestine. The colon exhibits the haustra, whereas the Kerckring’s fold is observed in the small intestine. During an examination, distinguishing the difference in peristalsis (lesser in the large bowel than in the small bowel) is also helpful. (B) The bowel has a 5-layer wall stratification: The 1st layer (hyperechoic) is the surface of the mucosa (superficial mucosa); 2nd layer (hypoechoic), the mucosa (deep mucosa) or muscularis mucosae; 3rd layer (hyperechoic), the submucosa; 4th layer (hypoechoic), the muscularis propria; and 5th layer (hyperechoic), the serosa.

Fig. 3. The landmark for identifying the sigmoid colon. At the left lower quadrant, the iliopsoas muscle and iliac blood vessels can be landmarks in identifying the sigmoid colon. The image is that of a patient with ulcerative colitis.

Fig. 4. Examination of the small intestine. (A) Ileocecal valve is identified while observing the ascending colon and cecum and then the terminal ileum can be followed from the ileocecal valve. At the right lower quadrant, the iliopsoas muscle and iliac blood vessels can be landmarks in identifying the sigmoid colon. This image is that of a patient with Crohn’s disease. (B) We screen the small bowel in the entire abdomen by moving the sonographic probe.
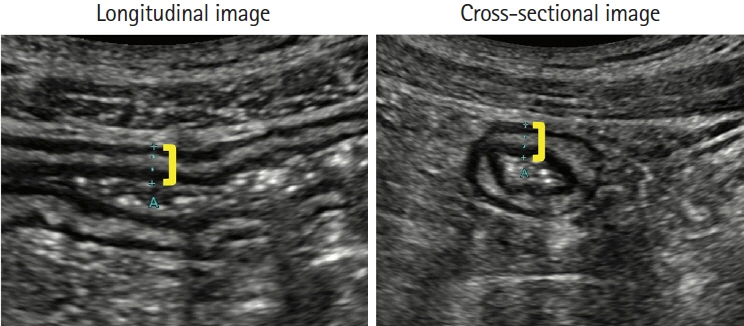
Fig. 5. Bowel wall thickness. The bowel wall thickness should be measured vertically to the wall (yellow line). These images are that of a patient with ulcerative colitis, which represents a thickened colon wall with a thickened submucosa.
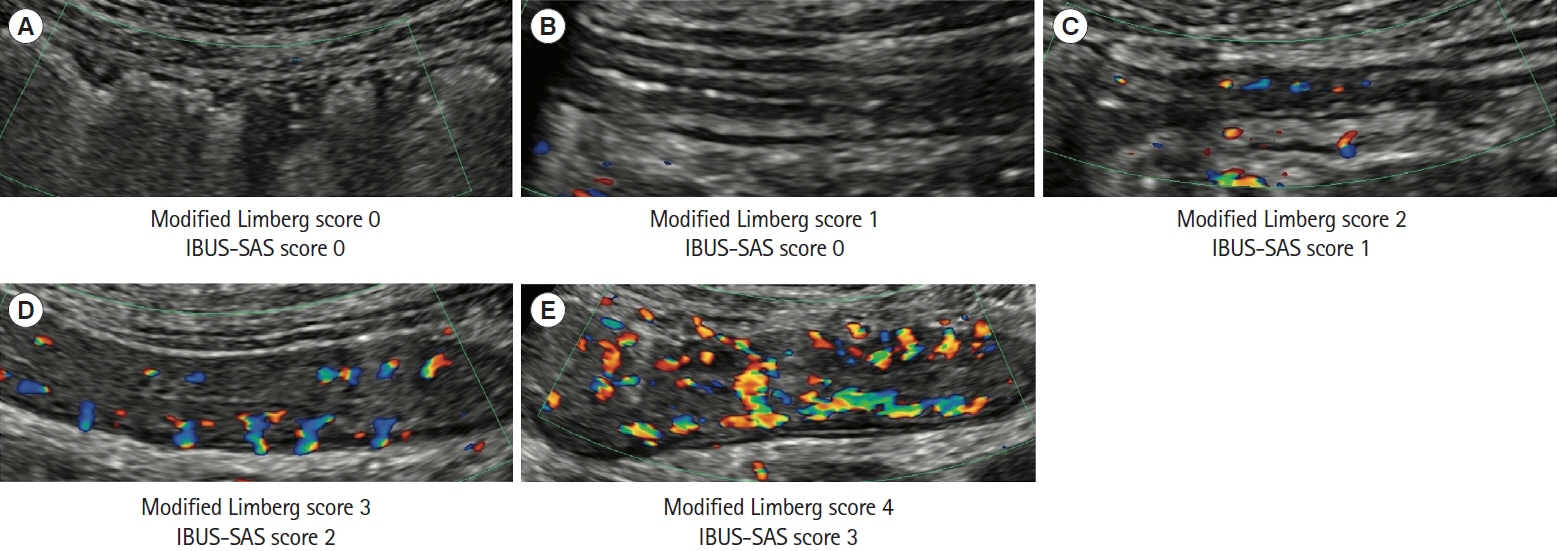
Fig. 6. Bowel wall flow. The bowel wall flow is generally assessed using color Doppler. The machine setting is crucial for appropriate examination. (A) Normal bowel wall thickness without color Doppler signal. (B) Thickened bowel wall without color Doppler signal. (C) Point-like, short color Doppler signals. (D) Linear-appearance color Doppler signals. (E) Long color Doppler signals extending the bowel wall and the surrounding mesenteric tissue. The velocity range of color Doppler for these images was 4.2 cm/s. IBUS-SAS, International Bowel Ultrasound Segmental Activity Score.
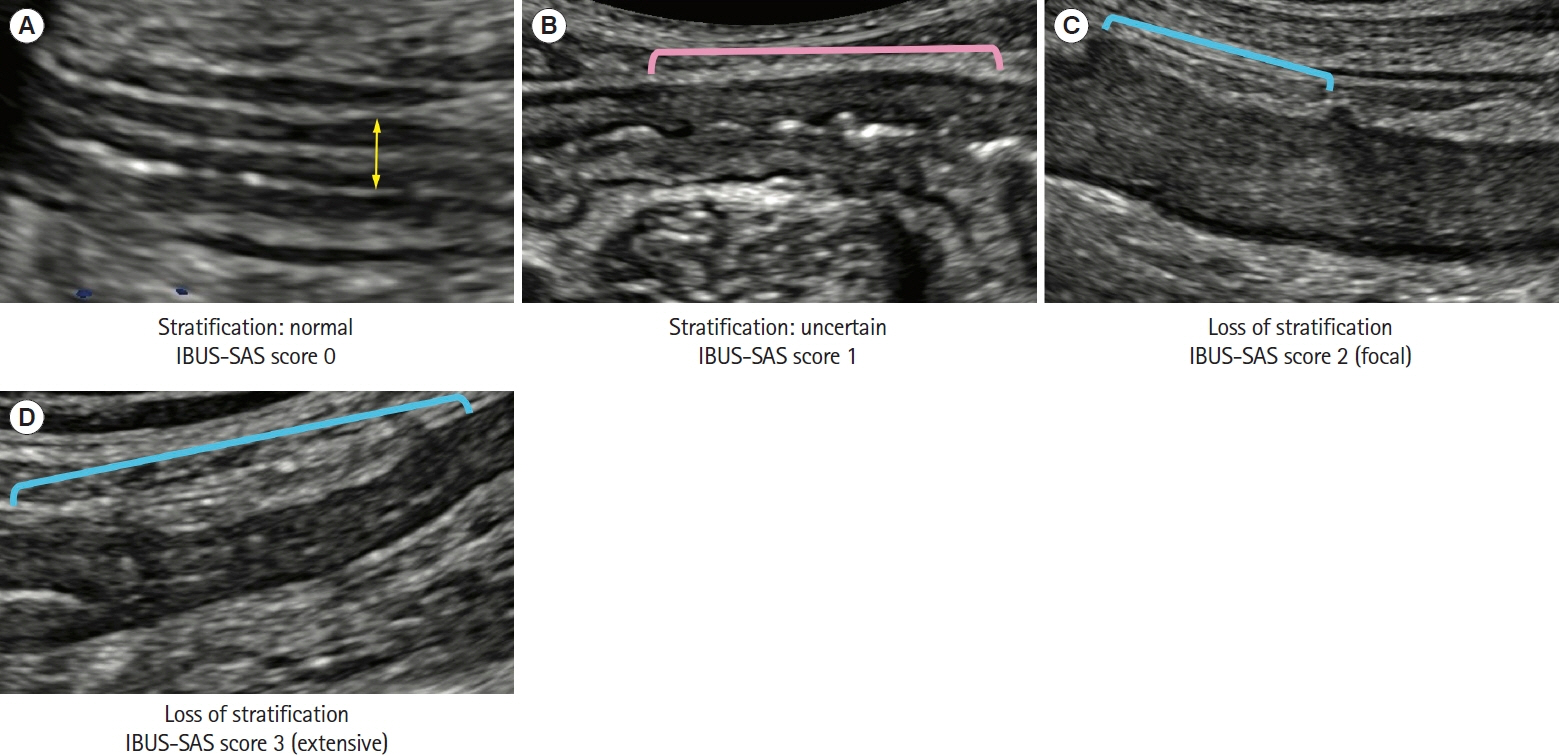
Fig. 7. Bowel wall stratification. (A) The normal 5-layer stratification. The yellow line represents bowel wall thickness. (B) The pink line indicates the area with uncertain bowel wall stratification. (C) The blue line indicates the area with loss of stratification. This image represents a focal loss of stratification (≤3 cm). (D) The blue line indicates the area with loss of stratification. This image represents an extensive loss of stratification (>3 cm). IBUS-SAS, International Bowel Ultrasound Segmental Activity Score.
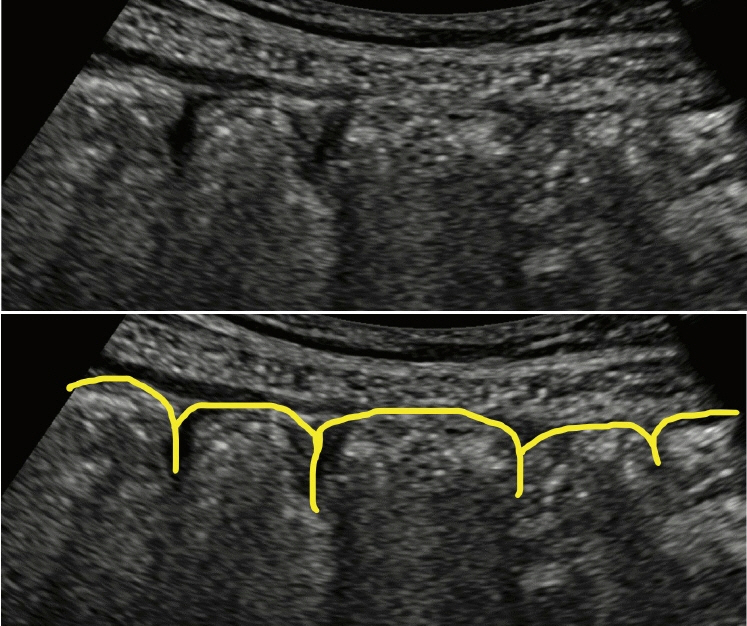
Fig. 8. Haustration of the colon. Both panels are identical sonographic images, and the yellow line in the lower panel indicates the haustration structure.
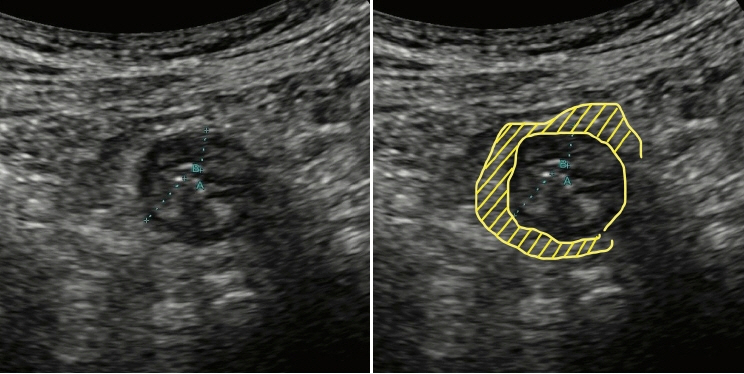
Fig. 9. Mesenteric proliferation (inflammation of mesenteric fat). Both panels are identical sonographic images, and the yellow area in the right panel indicates the hyperechogenic mesenteric tissue compared with the surrounding areas.

Fig. 10. Peri-intestinal lymph nodes. Both panels are identical sonographic images, and the yellow arrowheads in the right panel indicate lymph nodes surrounding the intestine.

Fig. 11. Thickened submucosa. The total bowel wall (yellow line) and the 3rd layer, i.e., the submucosa (pink line), are thickened. The ratio of the submucosa to the total bowel wall increases.
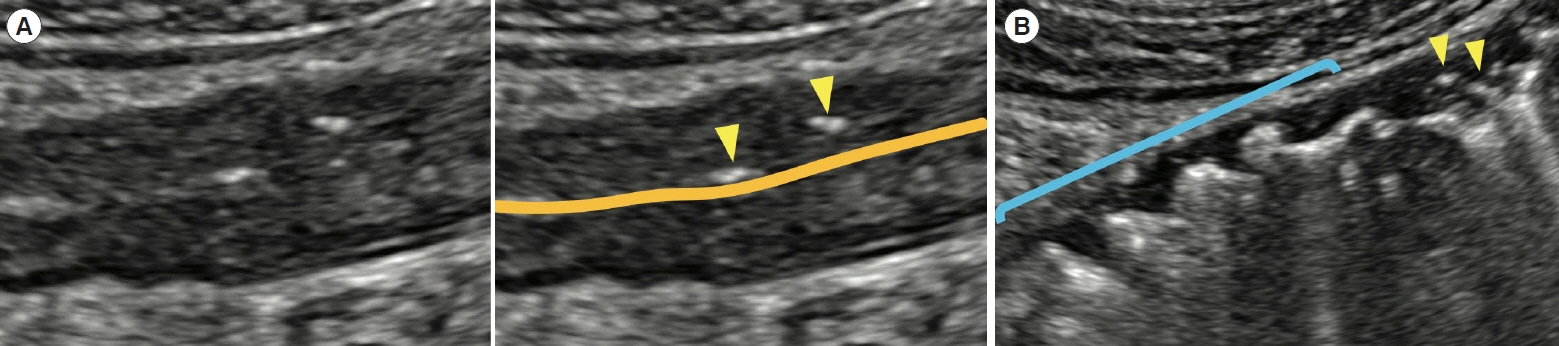
Fig. 12. Ulcer. (A) Both panels are identical sonographic images. The bottoms of the ulcers are observed inside the wall (yellow arrowheads). The orange line indicates the luminal surface. (B) The bowel wall appears thin due to the loss of wall tissues in the area with broad deep ulcers (blue line). The yellow arrowheads indicate ulcers.

Fig. 13. An example image of perineal intestinal ultrasound. The dorsal wall thickness of the rectum can be measured (pink line). This case with Crohn’s disease shows a perianal fistula (yellow arrowheads). The velocity range of the color Doppler for this image was 4.2 cm/s.

Fig. 14. Intestinal complications observed using ultrasound examinations. (A) The fistula between the terminal ileum and skin is shown (yellow arrowheads). An adhesion can be observed between the terminal ileum and cecum. (B) This perineal ultrasound image shows a perianal fistula (yellow arrowheads). The hyperechoic objects compatible with gas are observed in the fistula (blue arrowheads). (C) The hypoechoic area surrounded by yellow arrowheads is an abscess. Some hyperechoic objects compatible with gas (blue arrowheads) are observed inside the abscess. (D) This perianal ultrasound image shows a perianal abscess (surrounded by yellow arrowheads). Color Doppler signals are detected around the abscess. (E) Both panels are identical sonographic images. The dilation of the ileum (yellow arrowheads) occurs due to terminal ileum stenosis. The velocity range of color Doppler for images (B) and (D) was 4.2 cm/s.

Fig. 15. Hand-drawn report format in our facility. (A) Each format is used mainly for ulcerative colitis and Crohn’s disease. (B) An example illustration of the ileocecal area extracted from a hand-drawn report. In this patient with Crohn’s disease, inflammation is observed in the oral side of the ascending colon and the cecum, and these parts appear distorted with inflammatory fat and the local collection of ascites. With distortion, the ileocecal valve is observed at the ventral side of the cecum, and adhesion is detected between the terminal ileum and ventral side of the cecum (yellow arrowheads). The ileum is also inflamed, showing loss of stratification with mesenteric proliferation.
Reference
-
1. Windsor JW, Kaplan GG. Evolving epidemiology of IBD. Curr Gastroenterol Rep. 2019; 21:40.
Article2. Olén O, Askling J, Sachs MC, et al. Mortality in adult-onset and elderly-onset IBD: a nationwide register-based cohort study 1964-2014. Gut. 2020; 69:453–461.
Article3. Tsai L, Ma C, Dulai PS, et al. Contemporary risk of surgery in patients with ulcerative colitis and Crohn’s disease: a meta-analysis of population-based cohorts. Clin Gastroenterol Hepatol. 2021; 19:2031–2045.e11.
Article4. Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the selecting therapeutic targets in inflammatory bowel disease (STRIDE) initiative of the international organization for the study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021; 160:1570–1583.
Article5. Benitez JM, Meuwis MA, Reenaers C, Van Kemseke C, Meunier P, Louis E. Role of endoscopy, cross-sectional imaging and biomarkers in Crohn’s disease monitoring. Gut. 2013; 62:1806–1816.
Article6. Kucharzik T, Tielbeek J, Carter D, et al. ECCO-ESGAR topical review on optimizing reporting for cross-sectional imaging in inflammatory bowel disease. J Crohns Colitis. 2022; 16:523–543.
Article7. Maconi G, Nylund K, Ripolles T, et al. EFSUMB recommendations and clinical guidelines for intestinal ultrasound (GIUS) in inflammatory bowel diseases. Ultraschall Med. 2018; 39:304–317.
Article8. Maaser C, Sturm A, Vavricka SR, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 1: initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019; 13:144–164.
Article9. Sturm A, Maaser C, Calabrese E, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 2: IBD scores and general principles and technical aspects. J Crohns Colitis. 2019; 13:273–284.
Article10. Ilvemark JF, Hansen T, Goodsall TM, et al. Defining transabdominal intestinal ultrasound treatment response and remission in inflammatory bowel disease: systematic review and expert consensus statement. J Crohns Colitis. 2022; 16:554–580.
Article11. De Voogd F, Joshi H, Van Wassenaer E, Bots S, D’Haens G, Gecse K. Intestinal ultrasound to evaluate treatment response during pregnancy in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2022; 28:1045–1052.
Article12. Allocca M, Fiorino G, Bonifacio C, et al. Comparative accuracy of bowel ultrasound versus magnetic resonance enterography in combination with colonoscopy in assessing Crohn’s disease and guiding clinical decision-making. J Crohns Colitis. 2018; 12:1280–1287.
Article13. Kucharzik T, Wittig BM, Helwig U, et al. Use of intestinal ultrasound to monitor Crohn’s disease activity. Clin Gastroenterol Hepatol. 2017; 15:535–542.
Article14. Maaser C, Petersen F, Helwig U, et al. Intestinal ultrasound for monitoring therapeutic response in patients with ulcerative colitis: results from the TRUST&UC study. Gut. 2020; 69:1629–1636.
Article15. Kucharzik T, Wilkens R, D’Agostino MA, et al. Early ultrasound response and progressive transmural remission after treatment with ustekinumab in Crohn’s disease. Clin Gastroenterol Hepatol. 2023; 21:153–163.e12.16. Ilvemark JF, Wilkens R, Thielsen P, et al. Early intestinal ultrasound predicts intravenous corticosteroid response in hospitalised patients with severe ulcerative colitis. J Crohns Colitis. 2022; 16:1725–1734.
Article17. Sævik F, Eriksen R, Eide GE, Gilja OH, Nylund K. Development and validation of a simple ultrasound activity score for Crohn’s disease. J Crohns Colitis. 2021; 15:115–124.
Article18. Allocca M, Filippi E, Costantino A, et al. Milan ultrasound criteria are accurate in assessing disease activity in ulcerative colitis: external validation. United European Gastroenterol J. 2021; 9:438–442.
Article19. De Voogd F, Wilkens R, Gecse K, et al. A reliability study: strong inter-observer agreement of an expert panel for intestinal ultrasound in ulcerative colitis. J Crohns Colitis. 2021; 15:1284–1290.
Article20. Sagami S, Kobayashi T, Aihara K, et al. Transperineal ultrasound predicts endoscopic and histological healing in ulcerative colitis. Aliment Pharmacol Ther. 2020; 51:1373–1383.
Article21. Miyoshi J, Ozaki R, Yonezawa H, et al. Ratio of submucosal thickness to total bowel wall thickness as a new sonographic parameter to estimate endoscopic remission of ulcerative colitis. J Gastroenterol. 2022; 57:82–89.
Article22. Sagami S, Kobayashi T, Miyatani Y, et al. Accuracy of ultrasound for evaluation of colorectal segments in patients with inflammatory bowel diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2021; 19:908–921.e6.
Article23. Maconi G, Tonolini M, Monteleone M, et al. Transperineal perineal ultrasound versus magnetic resonance imaging in the assessment of perianal Crohn’s disease. Inflamm Bowel Dis. 2013; 19:2737–2743.
Article24. Sagami S, Kobayashi T, Aihara K, et al. Early improvement in bowel wall thickness on transperineal ultrasonography predicts treatment success in active ulcerative colitis. Aliment Pharmacol Ther. 2022; 55:1320–1329.
Article25. Novak KL, Nylund K, Maaser C, et al. Expert consensus on optimal acquisition and development of the international bowel ultrasound segmental activity score [IBUS-SAS]: a reliability and inter-rater variability study on intestinal ultrasonography in Crohn’s disease. J Crohns Colitis. 2021; 15:609–616.
Article26. Allocca M, Fiorino G, Bonovas S, et al. Accuracy of humanitas ultrasound criteria in assessing disease activity and severity in ulcerative colitis: a prospective study. J Crohns Colitis. 2018; 12:1385–1391.
Article27. Bots S, Nylund K, Löwenberg M, Gecse K, D’Haens G. Intestinal ultrasound to assess disease activity in ulcerative colitis: development of a novel UC-ultrasound index. J Crohns Colitis. 2021; 15:1264–1271.
Article28. Limberg B. Diagnosis of chronic inflammatory bowel disease by ultrasonography. Z Gastroenterol. 1999; 37:495–508.29. Gasche C, Moser G, Turetschek K, Schober E, Moeschl P, Oberhuber G. Transabdominal bowel sonography for the detection of intestinal complications in Crohn’s disease. Gut. 1999; 44:112–117.
Article30. Rieder F, Bettenworth D, Ma C, et al. An expert consensus to standardise definitions, diagnosis and treatment targets for anti-fibrotic stricture therapies in Crohn’s disease. Aliment Pharmacol Ther. 2018; 48:347–357.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Crohn’s disease at radiological imaging: focus on techniques and intestinal tract
- Can vitamin D supplementation help control inflammation in inflammatory bowel disease beyond its classical role in bone health?
- Intestinal Behcet's Disease: A True Inflammatory Bowel Disease or Merely an Intestinal Complication of Systemic Vasculitis?
- Artificial intelligence in inflammatory bowel disease: implications for clinical practice and future directions
- The Use of Transabdominal Ultrasound in Inflammatory Bowel Disease
