Hydration-induced rapid growth and regression after indirect revascularization of an anterior choroidal artery aneurysm associated with Moyamoya disease: A case report
- Affiliations
-
- 1Department of Neurosurgery, Armed Forces Capital Hospital, Seongnam, Korea
- 2Department of Neurosurgery, Korea University Anam Hospital, Seoul, Korea
- KMID: 2540810
- DOI: http://doi.org/10.7461/jcen.2022.E2022.02.002
Abstract
- The prevalence of aneurysm formation in adults with Moyamoya disease (MMD) is higher than that in the general population. The treatment strategy is often individualized based on the patient’s disease characteristics. A 22-year-old man was diagnosed with MMD after presenting a small thalamic intracerebral and subarachnoid hemorrhage in the quadrigeminal cistern. Cerebral angiography revealed a small aneurysm (2.42 mm) in the left anterior choroidal artery. Since the hemodynamics in the left hemisphere was compromised, an indirect bypass surgery was performed. The patient’s condition deteriorated postoperatively because of poor perfusion of the internal carotid artery, and massive hydration was required. During neurocritical care, the aneurysm increased in size (5.33 mm). An observation strategy was adopted because of the distal aneurysmal location and the high risk involved. Subsequently, the patient recovered, and newly developed collateral flow appeared from the external carotid artery. Additionally, a dramatic size reduction of the aneurysm (1.51 mm) was noticed. Our case suggests that MMD-related dissecting aneurysms on a distal cerebral artery, which present a high risk of embolization, could be managed by indirectly reducing the hemodynamic burden. Massive hydration in such cases should be avoided or balanced to avoid the risk of rapid growth and aneurysm rupture.
Figure
-
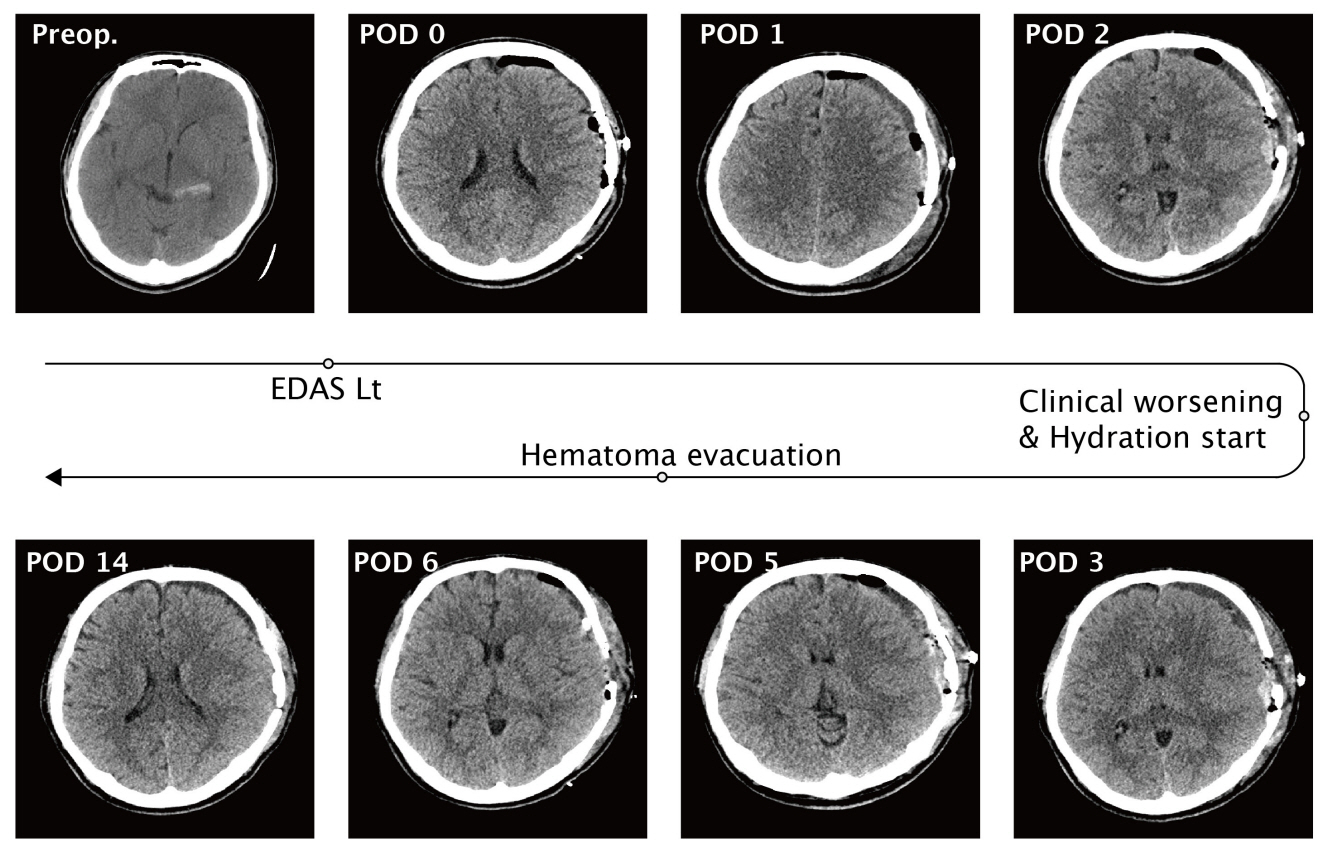
Fig. 1. Serial computed tomography (CT) images show from initial to Postoperative day 14 - Preoperative; Small amount of subarachnoid hemorrhage on the left quadrigeminal cistern on initial CT, Postoperative day 2; Clinical course got worsened (motor aphasia) and CT revealed the delayed postoperative hematoma on the epidural and subdural spaces, Postoperative day 6; Hematoma evacuation was performed due to the deep drowsy mentality with right hemiparesis (grade II). EDAS, encephalo-duro-arterio-synangiosis

Fig. 2. Chronological angiogram images – Preoperative; 2.42 mm sized saccular aneurysm was identified on his plexal segment of left anterior choroidal artery, Postoperative day 17, during massive hydration; Enlarged aneurysm of maximal diameter 5.33 mm, Postoperative day 35, after external carotid collateral formations; Dramatical size decrement of aneurysm.
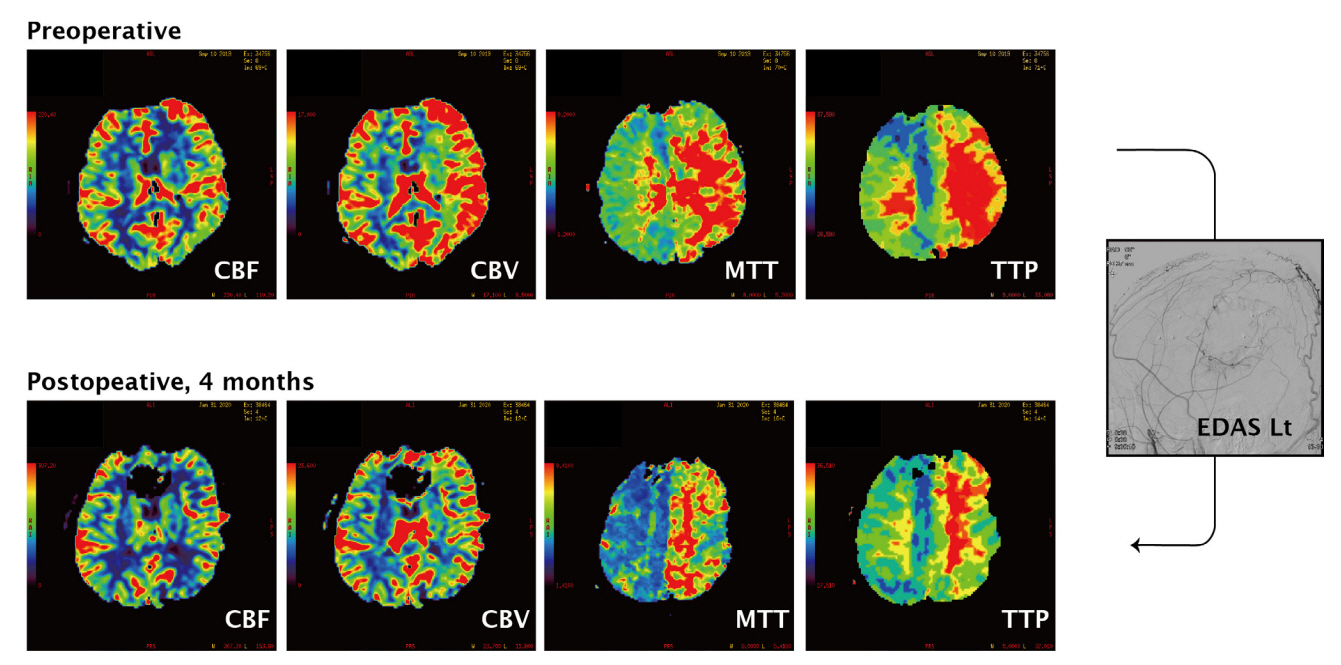
Fig. 3. Computed tomography perfusion (CTP) images – in the postoperative images, perfusion delay of the right hemisphere has been restored. CBF, cerebral blood flow; CBV, cerebral blood volume; MTT, mean transit time; TTP, time-to-peak; EDAS, encephalo-duro-arteriosynangiosis
Reference
-
1. Borota L, Marinkovic S, Bajic R, Kovacevic M. Intracranial aneurysms associated with Moyamoya disease. Neurol Med Chir (Tokyo). 1996; Dec. 36(12):860–4.2. Coughlin DJ, Miller CA, Schuette AJ. Treatment of Moyamoya disease and unruptured intracranial aneurysm in floatingharbor syndrome. World Neurosurg. 2017; Aug. 104:1049.3. Teixeira BCA, Cardoso-Demartini AA. Choreoathetosis in Moyamoya disease. World Neurosurg. 2021; Dec. 156:103–4.4. Duan L, Bao XY, Yang WZ, Shi WC, Li DS, Zhang ZS, et al. Moyamoya disease in China: its clinical features and outcomes. Stroke. 2012; Jan. 43(1):56–60.5. Kim JH, Kwon TH, Kim JH, Chong K, Yoon W. Intracranial aneurysms in adult Moyamoya disease. World Neurosurg. 2018; Jan. 109:e175–82.6. Kim S, Jang CK, Park EK, Shim KW, Kim DS, Chung J, et al. Clinical features and outcomes of intracranial aneurysm associated with Moyamoya disease. J Clin Neurol. 2020; Oct. 16(4):624–32.7. Lee CY. Embolization with NBCA for ruptured aneurysm located in the Moyamoya-like collateral network associated with isolated middle cerebral artery occlusion. Asian J Neurosurg. 2018; Oct-Dec. 13(4):1236–8.8. Matsushima Y, Qian L, Aoyagi M. Clin Neurol Neurosurg. Asian J Neurosurg. 1997; Oct. 99 Suppl 2:S19–22.9. Takahashi JC, Miyamoto S. Moyamoya disease: recent progress and outlook. Neurol Med Chir (Tokyo). 2010; 50(9):824–32.10. Yamada H, Saga I, Kojima A, Horiguchi T. Short-term spontaneous resolution of ruptured peripheral aneurysm in Moyamoya disease. World Neurosurg. 2019; Jun. 126:247–51.11. Zhang L, Xu K, Zhang Y, Wang X, Yu J. Treatment strategies for aneurysms associated with Moyamoya disease. Int J Med Sci. 2015; Feb. 12(3):234–42.12. Zhao X, Wang X, Wang M, Meng Q, Wang C. Treatment strategies of ruptured intracranial aneurysms associated with Moyamoya disease. Br J Neurosurg. 2021; Apr. 35(2):209–15.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transposition of Anterior Choroidal Artery and Posterior Communicating Artery Origin
- Endovascular Management of Peripheral Lateral Posterior Choroidal Artery Aneurysm Associated with Moyamoya disease: Case Report and Review of the Literature
- Extravasation from the Distal Anterior Choroidal Artery Aneurysm in Moyamoya Patient during Computed Tomographic Angiography
- Neuroimaging Diagnosis and Treatment of Moyamoya Disease
- Oculomotor Nerve Palsy due to Ruptured Multiple Anterior Choroidal Artery Aneurysms
