Bronchoesophageal fistula in a patient with Crohn’s disease receiving anti-tumor necrosis factor therapy
- Affiliations
-
- 1Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 3Department of Pulmonology and Critical Care Medicine, Asan medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Inflammatory Bowel Disease Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2540742
- DOI: http://doi.org/10.5946/ce.2021.215
Abstract
- Tuberculosis is an adverse event in patients with Crohn’s disease receiving anti-tumor necrosis factor (TNF) therapy. However, tuberculosis presenting as a bronchoesophageal fistula (BEF) is rare. We report a case of tuberculosis and BEF in a patient with Crohn’s disease who received anti-TNF therapy. A 33-year-old Korean woman developed fever and cough 2 months after initiation of anti-TNF therapy. And the symptoms persisted for 1 months, so she visited the emergency room. Chest computed tomography was performed upon visiting the emergency room, which showed BEF with aspiration pneumonia. Esophagogastroduodenoscopy with biopsy and endobronchial ultrasound with transbronchial needle aspiration confirmed that the cause of BEF was tuberculosis. Anti-tuberculosis medications were administered, and esophageal stent insertion through endoscopy was performed to manage the BEF. However, the patient’s condition did not improve; therefore, fistulectomy with primary closure was performed. After fistulectomy, the anastomosis site healing was delayed due to severe inflammation, a second esophageal stent and gastrostomy tube were inserted. Nine months after the diagnosis, the fistula disappeared without recurrence, and the esophageal stent and gastrostomy tube were removed.
Figure
-
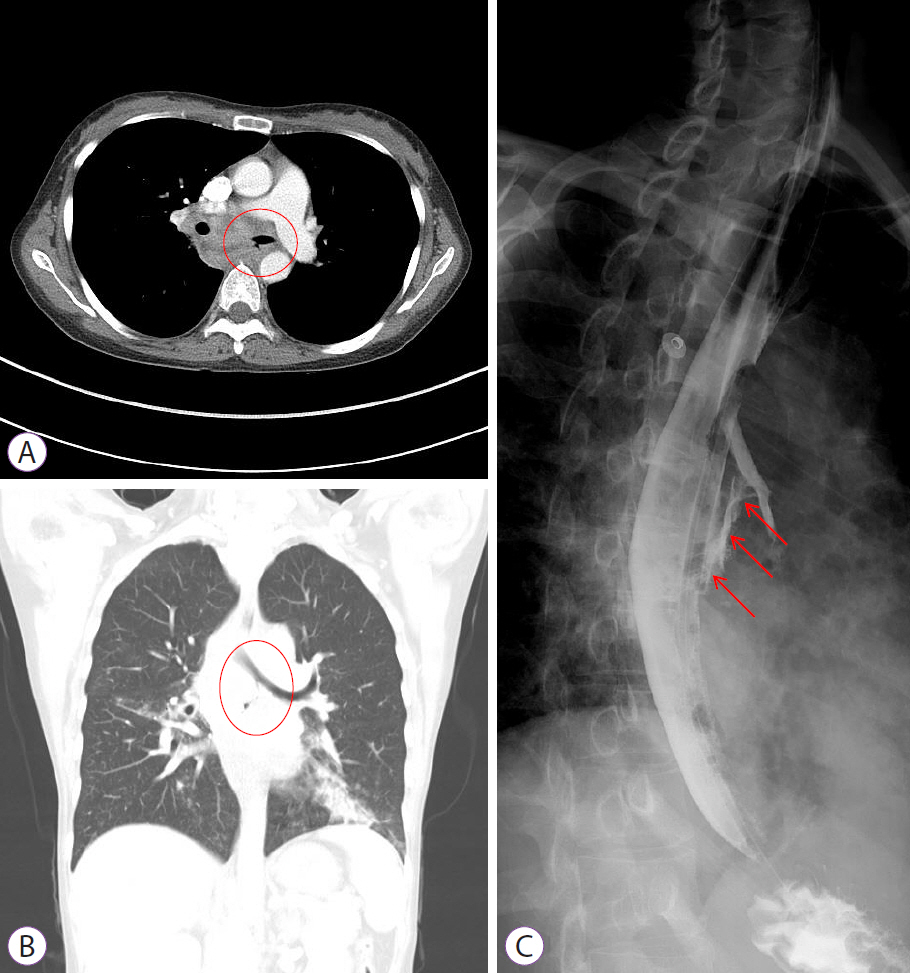
Fig. 1. (A, B) Chest computed tomography shows an air cleft between the esophagus and the left main bronchus (in the red circles), suggesting bronchoesophageal fistula and aspiration pneumonia. (C) Esophagography shows contrast media leakage from the esophagus to the left bronchus (red arrows).

Fig. 2. (A, B) Esophagogastroduodenoscopy shows a deep ulcer (in the green circles) in the esophagus at 28 to 32 cm from upper incisor.
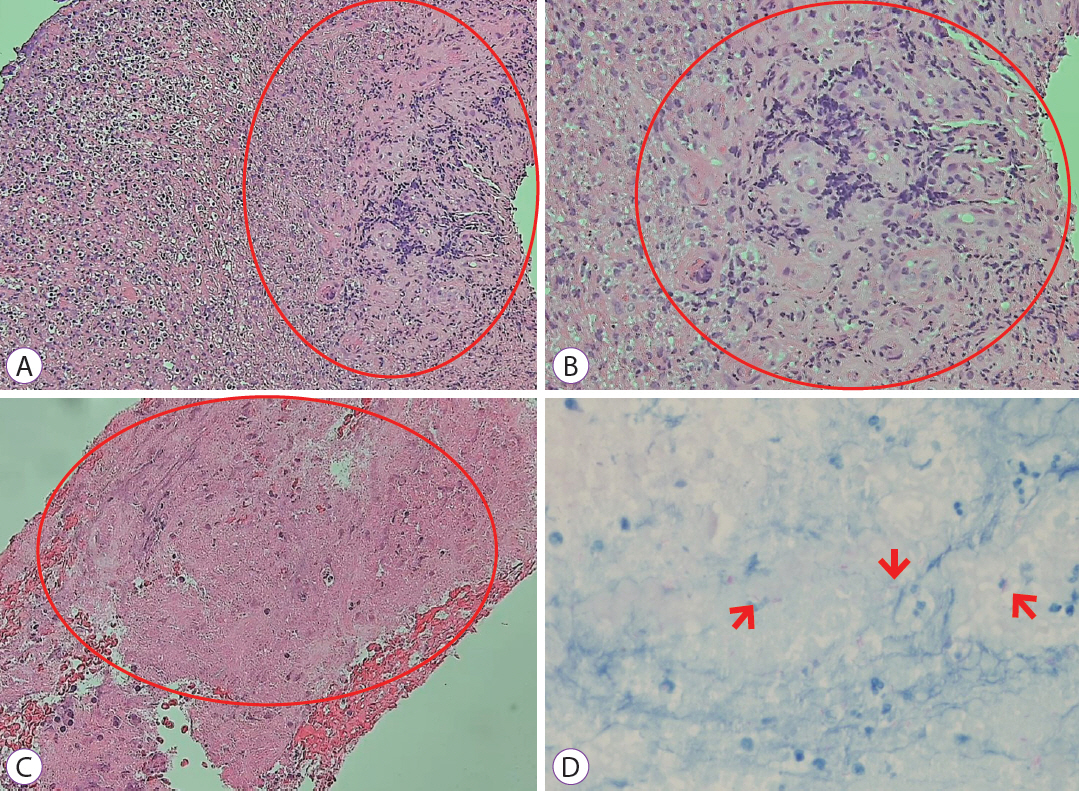
Fig. 3. (A, B) Esophagogatroduodenoscopic biopsy shows granulomatous inflammation with granulation tissue and marked necrosis (in the red circles). Hematoxylin and eosin stain: (A) ×100, (B) ×200. (C, D) Endobronchial ultrasound with transbronchial needle aspiration shows chronic granulomatous inflammation with necrosis (in the red circle), and many acid-fast positive bacilli (red arrows) are identified by acid-fast bacilli staining. (C) Hematoxylin and eosin stain ×200. (D) Acid-fest bacilli stain ×400.
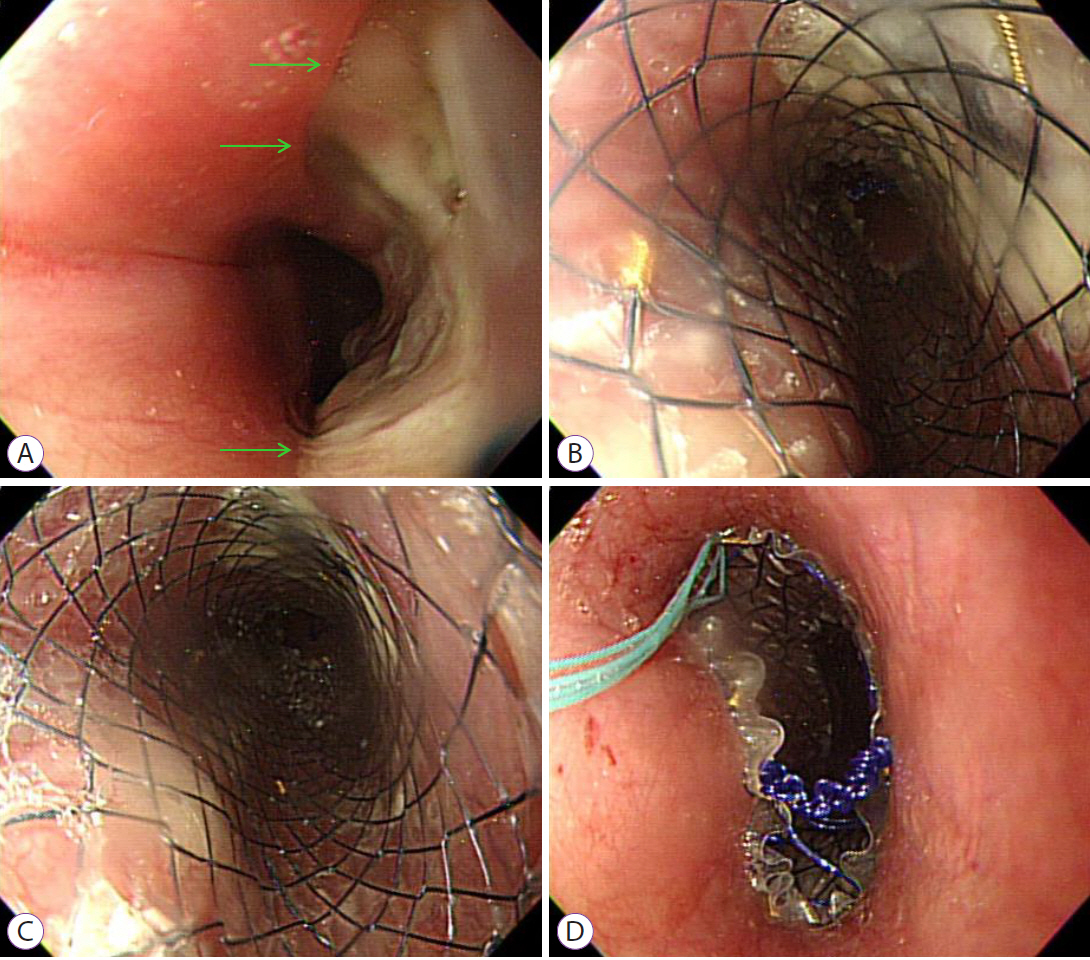
Fig. 4. (A) An esophageal ulcer (green arrows) was seen on esophagogastroduodenoscopy. (B–D) A covered esophageal stent was inserted.

Fig. 5. (A, B) Esophagography 2 months after diagnosis shows persistent contrast media leakage from the esophagus to the left bronchus (red arrows). (C, D) Esophagography 9 months after diagnosis shows no contrast media leakage.
Reference
-
1. Park SH, Kim YJ, Rhee KH, et al. A 30-year trend analysis in the epidemiology of inflammatory bowel disease in the Songpa-Kangdong district of Seoul, Korea in 1986-2015. J Crohns Colitis. 2019; 13:1410–1417.2. Kaibullayeva J, Ualiyeva A, Oshibayeva A, et al. Prevalence and patient awareness of inflammatory bowel disease in Kazakhstan: a cross-sectional study. Intest Res. 2020; 18:430–437.3. Yen HH, Weng MT, Tung CC, et al. Epidemiological trend in inflammatory bowel disease in Taiwan from 2001 to 2015: a nationwide population-based study. Intest Res. 2019; 17:54–62.4. Wilkens R, Novak KL, Maaser C, et al. Relevance of monitoring transmural disease activity in patients with Crohn’s disease: current status and future perspectives. Therap Adv Gastroenterol. 2021; 14:17562848211006672.5. Hong SW, Ye BD. The first step to unveil the epidemiology of inflammatory bowel disease in Central Asia. Intest Res. 2020; 18:345–346.6. Park DI, Hisamatsu T, Chen M, et al. Asian organization for Crohn’s and colitis and Asia Pacific Association of Gastroenterology consensus on tuberculosis infection in patients with inflammatory bowel disease receiving anti-tumor necrosis factor treatment. Part 1: risk assessment. Intest Res. 2018; 16:4–16.7. Spalding AR, Burney DP, Richie RE. Acquired benign bronchoesophageal fistulas in the adult. Ann Thorac Surg. 1979; 28:378–383.8. Balazs A, Kupcsulik PK, Galambos Z. Esophagorespiratory fistulas of tumorous origin. Non-operative management of 264 cases in a 20-year period. Eur J Cardiothorac Surg. 2008; 34:1103–1107.9. Holder TM, Cloud DT, Lewis JE, et al. Esophageal atresia and tracheoesophageal fistula. A survey of its members by the surgical section of the american academy of pediatrics. Pediatrics. 1964; 34:542–549.10. Desai P, Mayenkar P, Northrup TF, et al. Bronchoesophageal fistula due to esophageal tuberculosis. Case Rep Infect Dis. 2019; 2019:6537437.11. Aissaoui H, Louvel D, Drak Alsibai K. SARS-CoV-2 and mycobacterium tuberculosis coinfection: a case of unusual bronchoesophageal fistula. J Clin Tuberc Other Mycobact Dis. 2021; 24:100247.12. Clarke BW, Cassara JE, Morgan DR. Crohn’s disease of the esophagus with esophagobronchial fistula formation: a case report and review of the literature. Gastrointest Endosc. 2010; 71:207–209.13. Saadah OI, Fallatah KB, Baumann C, et al. Histologically confirmed upper gastrointestinal Crohn’s disease: is it rare or are we just not searching hard enough? Intest Res. 2020; 18:210–218.14. Devbhandari MP, Raco L, Hendrickse MT, et al. Congenital bronchoesophageal fistula in a patient with Crohn’s disease: a cautionary tale. Ann Thorac Surg. 2005; 79:1776–1777.15. Kato H, Yoshikawa M, Saito T, et al. Congenital bronchoesophageal fistula with Crohn’s disease in an adult: report of a case. Surg Today. 2001; 31:446–449.16. Agarwal A, Kedia S, Jain S, et al. High risk of tuberculosis during infliximab therapy despite tuberculosis screening in inflammatory bowel disease patients in India. Intest Res. 2018; 16:588–598.17. Alrajhi S, Germain P, Martel M, et al. Concordance between tuberculin skin test and interferon-gamma release assay for latent tuberculosis screening in inflammatory bowel disease. Intest Res. 2020; 18:306–314.18. Bibas BJ, Cardoso PFG, Minamoto H, et al. Surgery for intrathoracic tracheoesophageal and bronchoesophageal fistula. Ann Transl Med. 2018; 6:210.19. Spaander MCW, van der Bogt RD, Baron TH, et al. Esophageal stenting for benign and malignant disease: European Society of Gastrointestinal Endoscopy (ESGE) guideline-update 2021. Endoscopy. 2021; 53:751–762.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative use of anti-tumor necrosis factor therapy in Crohn's disease: promises and pitfalls
- Recent Trends of Infliximab Treatment for Crohn's Disease
- Anti-tumor Necrosis Factor Therapy for Crohn Disease: Friend or Foe to the Surgeon?
- A Pityrosporum Fungal Infection Following Infliximab Therapy in a Crohn's Disease Patient
- A Bronchoesophageal Fistula Detected by Air Leaking Sound after Intubation
