Cardiovasc Prev Pharmacother.
2023 Jan;5(1):24-34. 10.36011/cpp.2023.5.e3.
Modifiable risk factors for coronary artery disease in the Indonesian population: a nested case-control study
- Affiliations
-
- 1Department of Cardiology and Vascular Medicine, Dr. Sardjito Hospital, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
- 2Department of Histology and Cell Biology, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
- 3Health and Demographic Surveillance System (HDSS) Sleman, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
- 4Department of Public Health Science, Faculty of Sport Science, Universitas Negeri Semarang, Semarang, Indonesia
- 5Department of Health Behavior, Environment and Social Medicine, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
- KMID: 2540037
- DOI: http://doi.org/10.36011/cpp.2023.5.e3
Abstract
- Background
There is a lack of data on modifiable coronary artery disease (CAD) risk factors in the Indonesian population, hindering the implementation of assessments and prevention programs in this population. This study investigated modifiable risk factors for CAD among Indonesians by comparing them between CAD-proven patients and healthy subjects from a similar population.
Methods
In this nested, matched case-control study, the cases were patients from a referral hospital in Yogyakarta, Indonesia and the controls were respondents in a population surveillance system in Yogyakarta, Indonesia. The cases were 421 patients who had undergone coronary angiography, showing significant CAD. The sex- and age-matched controls were 842 respondents from the Universitas Gadjah Mada Health and Health and Demographic Surveillance System Sleman who indicated no CAD presence on a questionnaire. The modifiable CAD risk factors compared between cases and controls were diabetes mellitus, hypertension, central obesity, smoking history, physical inactivity, and less fruit and vegetable intake. A multivariate regression model was applied to determine independent modifiable risk factors for CAD, expressed as adjusted odds ratios (AORs).
Results
A multivariate analysis model of 1,263 subjects including all modifiable risk factors indicated that diabetes mellitus (AOR, 3.32; 95% confidence interval [CI], 2.09–5.28), hypertension (AOR, 2.52; 95% CI, 1.76–3.60), former smoking (AOR, 4.18; 95% CI, 2.73–6.39), physical inactivity (AOR, 15.91; 95% CI, 10.13–24.99), and less fruit and vegetable intake (AOR, 5.42; 95% CI, 2.84–10.34) independently and significantly emerged as risk factors for CAD.
Conclusions
Hypertension, diabetes mellitus, former smoking, physical inactivity, and less fruit and vegetable intake were independent and significant modifiable risk factors for CAD in the Indonesian population.
Keyword
Figure
-
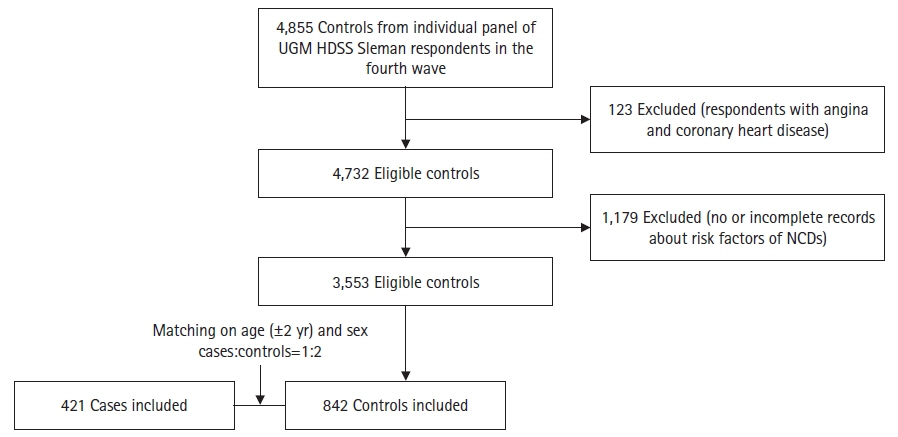
Fig. 1. Flowchart depicting the selection process of controls, where controls were matched for age (±2 years old) and sex with the cases. The ratio of cases to age- and sex-matched controls was 1:2. HDSS, Health and Demographic Surveillance System; NCD, noncommunicable disease.
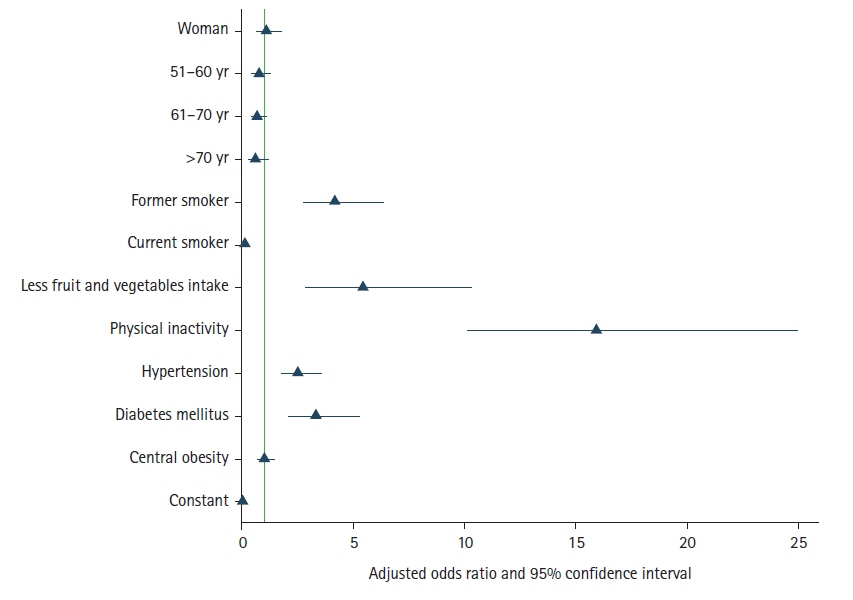
Fig. 2. Results of the multivariate analysis showing the associations between risk factors and coronary artery disease. Modifiable risk factors—namely, clinical risk factors (such as hypertension and diabetes mellitus, but not central obesity) and lifestyle-related risk factors (such as former smoking, physical inactivity, and less fruit and vegetable intake)—were independent and significant risk factors for coronary artery disease.
Reference
-
1. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017; 390:1151–210.2. GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017; 390:1260–344.3. Institute of Health Metrics and Evaluation (IHME). Indonesia [Internet]. IHME; 2019. Available from: https://www.healthdata.org/indonesia.4. Maharani A, Praveen D, Oceandy D, Tampubolon G, Patel A. Cardiovascular disease risk factor prevalence and estimated 10-year cardiovascular risk scores in Indonesia: the SMARThealth extend study. PLoS One. 2019; 14:e0215219.5. Authors/Task Force Members, Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur J Prev Cardiol. 2016; 23:NP1–96.6. Adisasmito W, Amir V, Atin A, Megraini A, Kusuma D. Geographic and socioeconomic disparity in cardiovascular risk factors in Indonesia: analysis of the basic health research 2018. BMC Public Health. 2020; 20:1004.7. BPS-Statistics Indonesia. Statistical yearbook of Indonesia 2018. BPS-Statistics Indonesia; 2018.8. Dewi FS, Choiriyyah I, Indriyani C, Wahab A, Lazuardi L, Nugroho A, et al. Designing and collecting data for a longitudinal study: the Sleman Health and Demographic Surveillance System (HDSS). Scand J Public Health. 2018; 46:704–10.9. Nemeth R. Sampling design of health surveys: household as a sampling unit. LIS working paper series no. 358. Luxembourg Income Study; 2003.10. Rose G, McCartney P, Reid DD. Self-administration of a questionnaire on chest pain and intermittent claudication. Br J Prev Soc Med. 1977; 31:42–8.11. Hartopo AB, Fachiroh J, Puspitawati I, Dewi FS. Serum endothelin-1 level positively correlates with waist and hip circumferences in stable coronary artery disease patients. Rev Cardiovasc Med. 2021; 22:919–24.12. Harbuwono DS, Pramono LA, Yunir E, Subekti I. Obesity and central obesity in Indonesia: evidence from a national health survey. Med J Indones. 2018; 27:114–20.13. World Health Organization (WHO). WHO STEPS instrument for chronic disease. WHO; 2009.14. Defianna SR, Santosa A, Probandari A, Dewi FS. Gender differences in prevalence and risk factors for hypertension among adult populations: a cross-sectional study in Indonesia. Int J Environ Res Public Health. 2021; 18:6259.15. World Health Organization (WHO). The WHO STEPS surveillance manual. WHO; 2008.16. World Health Organization (WHO). Global physical activity questionnaire (GPAQ) analysis guide. WHO; 2012.17. Hussain MA, Al Mamun A, Peters SA, Woodward M, Huxley RR. The burden of cardiovascular disease attributable to major modifiable risk factors in Indonesia. J Epidemiol. 2016; 26:515–21.18. Martiniuk AL, Lee CM, Lawes CM, Ueshima H, Suh I, Lam TH, et al. Hypertension: its prevalence and population-attributable fraction for mortality from cardiovascular disease in the Asia-Pacific region. J Hypertens. 2007; 25:73–9.19. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004; 364:937–52.20. International Diabetes Federation (IDF). IDF diabetes atlas. IDF; 2017.21. Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endocrinol. 2015; 3:105–13.22. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012; 380:219–29.23. Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016; 67:1–12.24. Agency of Health Research and Development (Indonesia). Indonesia basic health research (RISKESDAS) 2018. Ministry of Health (Indonesia); 2018.25. Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019; 74:e177–232.26. Wu Y, Qian Y, Pan Y, Li P, Yang J, Ye X, et al. Association between dietary fiber intake and risk of coronary heart disease: a meta-analysis. Clin Nutr. 2015; 34:603–11.27. Arsyad DS, Westerink J, Cramer MJ, Ansar J, Wahiduddin , Visseren FL, et al. Modifiable risk factors in adults with and without prior cardiovascular disease: findings from the Indonesian National Basic Health Research. BMC Public Health. 2022; 22:660.28. Teo KK, Ounpuu S, Hawken S, Pandey MR, Valentin V, Hunt D, et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006; 368:647–58.29. Lv X, Sun J, Bi Y, Xu M, Lu J, Zhao L, et al. Risk of all-cause mortality and cardiovascular disease associated with secondhand smoke exposure: a systematic review and meta-analysis. Int J Cardiol. 2015; 199:106–15.30. Mons U, Muezzinler A, Gellert C, Schottker B, Abnet CC, Bobak M, et al. Impact of smoking and smoking cessation on cardiovascular events and mortality among older adults: meta-analysis of individual participant data from prospective cohort studies of the CHANCES consortium. BMJ. 2015; 350:h1551.31. Pearce N. Analysis of matched case-control studies. BMJ. 2016; 352:i969.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Identifying Latent Classes of Risk Factors for Coronary Artery Disease
- Effects Of Self-care Health Behaviors On Quality Of Life Mediated By Cardiovascular Risk Factors Among Individuals With Coronary Artery Disease: A Structural Equation Modeling Approach
- Evaluation of Lipoprotein(a) as a Risk Factor for Coronary Artery Disease
- Survey result on the prevalence of hyperlipidemia and other risk factors of coronary artery disease among Korean population
- Applicability and Program Effects of Tai Chi Exercise in Outpatients with Coronary Artery Disease
