Modified Pulvertaft orthogonal passing-through suture technique: a preliminary study
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University Hospital, Seoul, Korea
- 2Department of Orthopedic Surgery, Dong-A University Hospital, Busan, Korea
- KMID: 2540027
- DOI: http://doi.org/10.12790/ahm.22.0037
Abstract
- Purpose
If the primary suture is difficult due to the large size of a tendon defect, reconstruction of the defective tendon is attempted through tendon transfer or tendon graft. The Pulvertaft technique is most commonly used, but it increases bulk and friction, and it could cause adhesion formation. In order to overcome these problems, we aimed to introduce a new technique.
Methods
We retrospectively reviewed 22 patients who underwent tendon reconstruction using the modified Pulvertaft technique due to tendon defects from January 2016 to December 2021. An abbreviated version of the original DASH (Disabilities of Arm, Shoulder and Hand) outcome measure (QuickDASH) was measured 3 months after surgery. Until the final follow-up observation, tendon rerupture, infection, tendon-related complications (quadriga effect, motion limitation due to bulky size of the suture site), and contracture were measured. QuickDASH was compared according to the cause of the tendon defect and the type of operation using the Mann-Whitney test.
Results
The mean QuickDASH score measured 3 months after surgery was 10.42±7.83. No statistically significant difference in the QuickDASH score was found between patients who underwent tendon transfer and those who underwent tendon grafts (p=0.988). Rerupture occurred in 1 case, and there were no cases of infection, tendon-related complications (quadriga effect, motion limitation due to bulky size of the suture site), or contracture.
Conclusion
The orthogonal passing-through suture technique could be a new alternative to the tendon reconstruction technique.
Keyword
Figure
-

Fig. 1. (A) Conventional Pulvertaft method. (B) The blue and red tendons are connected by the modified orthogonal passing-through Pulveraft suture method.
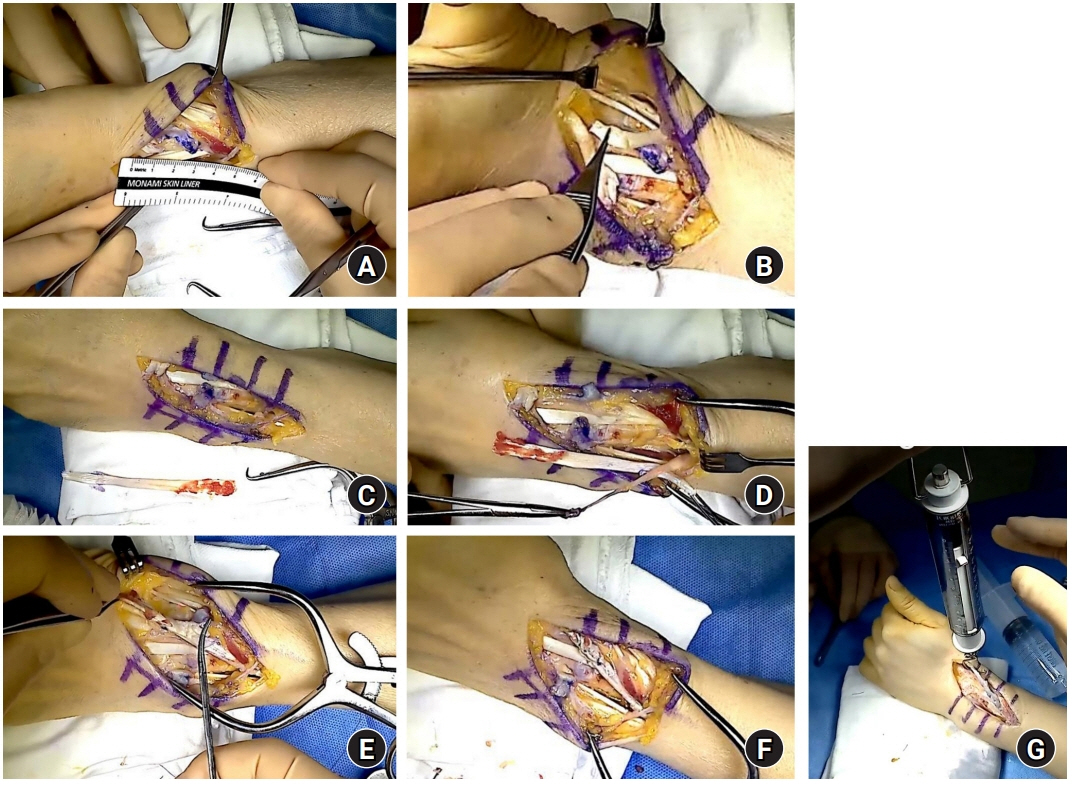
Fig. 2. (A) Residual portion of the proximal and distal end of the ruptured extensor pollicis longus. (B) Harvesting slip of the abductor pollicis longus (APL) for donor graft. (C) Harvested tendon slip of the APL. (D) Pulvertaft suture between the donor graft and proximal stump. (E) Pulvertaft suture between the donor graft and distal stump. (F) Image of the completed tendon graft. (G) Measuring the tensile strength of tendon graft using a suspension scale.
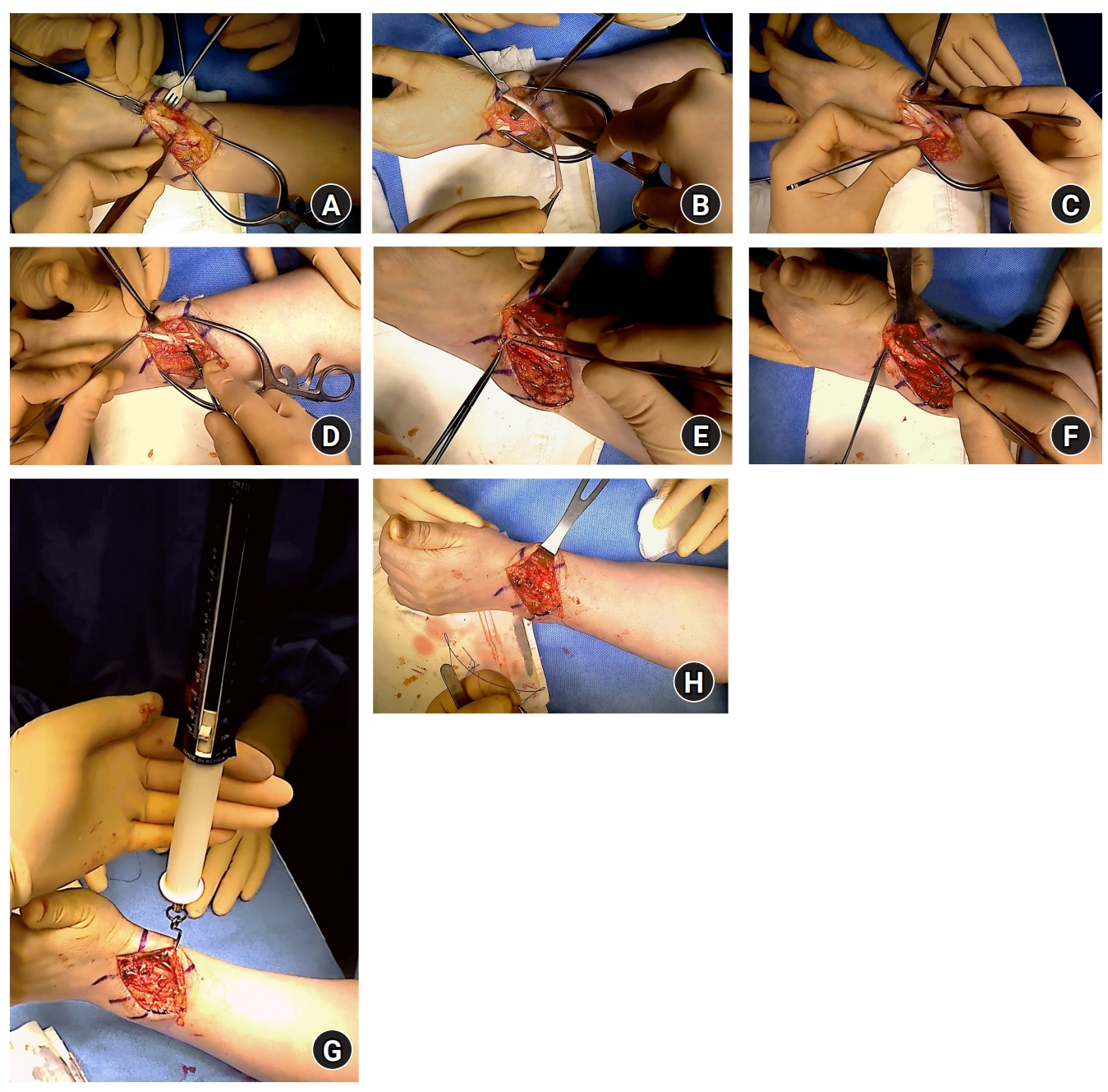
Fig. 3. (A) Ruptured proximal end of the extensor pollicis longus (EPL). (B) Harvesting a slip of the abductor pollicis longus tendon for tendon transfer. (C) Creating a hole for passage of the first Pulvertaft suture. (D) The second Pulvertaft suture. (E) The third Pulvertaft suture. (F) The fourth Pulvertaft suture. (G) Test of sufficient tension for resistance. (H) Completed EPL reconstruction using the Pulvertaft suture.
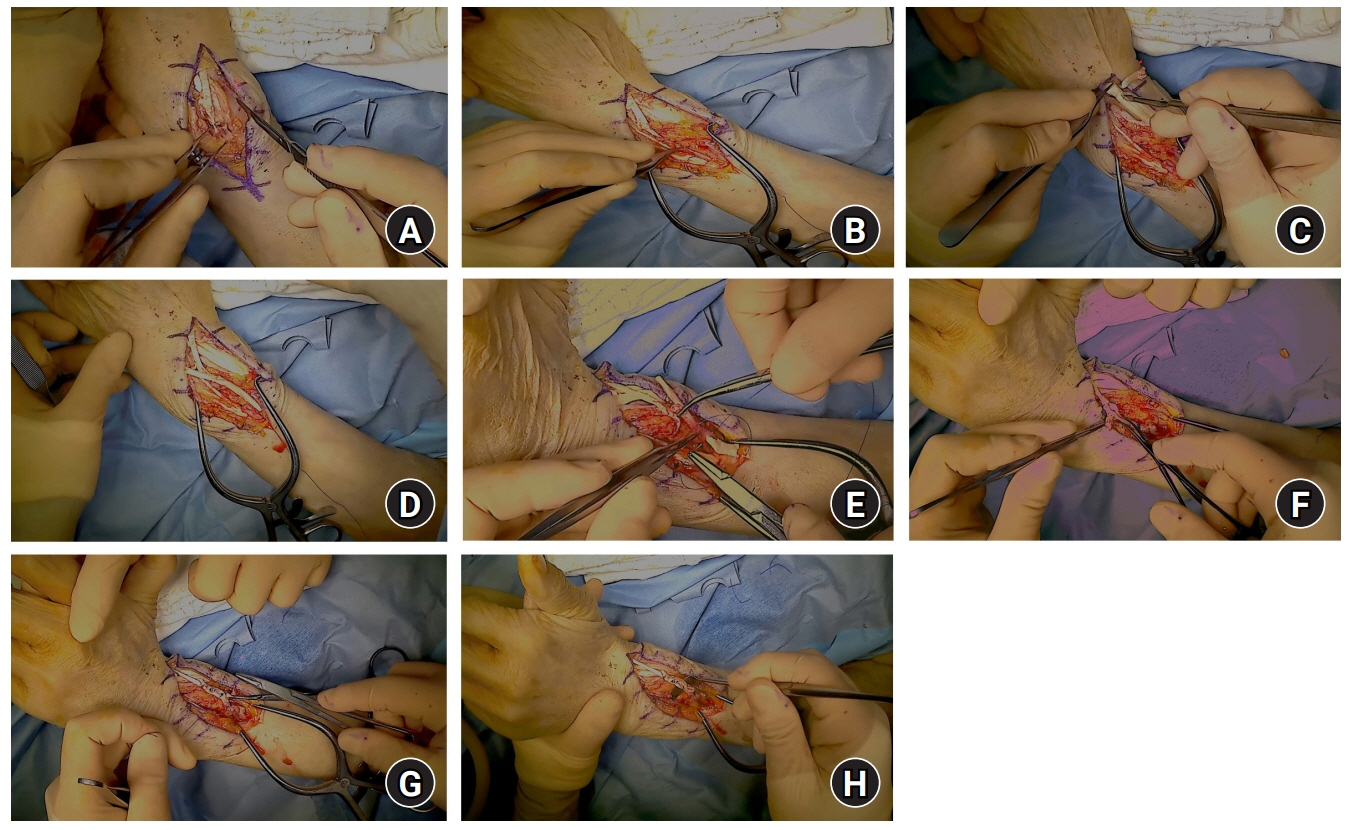
Fig. 4. (A) Proximal end of the ruptured extensor pollicis longus (EPL). (B) Wide gap between both ruptured ends of the EPL, making direct repair impossible. (C) Harvesting a slip of the extensor carpi radialis brevis by longitudinal cleavage for the donor tendon. (D) Approximation of the proximal and distal ends of the ruptured EPL and donor tendon. (E) Suture between the proximal end of EPL and the graft tendon using the Pulvertaft method. (F) Suture between the distal end of the EPL and the graft tendon using the Pulvertaft method. (G) The third suture between the ruptured EPL and the graft tendon using the orthogonal Pulvertaft method. (H) Completed EPL reconstruction using a Pulvertaft suture (the fourth suture).
Reference
-
References
1. Rivlin M, Eberlin KR, Kachooei AR, et al. Side-to-side versus Pulvertaft extensor tenorrhaphy: a biomechanical study. J Hand Surg Am. 2016; 41:e393–7.2. Jeon SH, Chung MS, Baek GH, Lee YH, Kim SH, Gong HS. Comparison of loop-tendon versus end-weave methods for tendon transfer or grafting in rabbits. J Hand Surg Am. 2009; 34:1074–9.3. Kulikov YI, Dodd S, Gheduzzi S, Miles AW, Giddins GE. An in vitro biomechanical study comparing the spiral linking technique against the pulvertaft weave for tendon repair. J Hand Surg Eur Vol. 2007; 32:377–81.4. Tanaka T, Zhao C, Ettema AM, Zobitz ME, An KN, Amadio PC. Tensile strength of a new suture for fixation of tendon grafts when using a weave technique. J Hand Surg Am. 2006; 31:982–6.5. Fuchs SP, Walbeehm ET, Hovius SE. Biomechanical evaluation of the Pulvertaft versus the ‘wrap around’ tendon suture technique. J Hand Surg Eur Vol. 2011; 36:461–6.6. Pulvertaft RG. Tendon grafts for flexor tendon injuries in the fingers and thumb; a study of technique and results. J Bone Joint Surg Br. 1956; 38-B:175–94.7. Bidic SM, Varshney A, Ruff MD, Orenstein HH. Biomechanical comparison of lasso, Pulvertaft weave, and side-by-side tendon repairs. Plast Reconstr Surg. 2009; 124:567–71.8. Vincken NL, Lauwers TM, van der Hulst RR. Biomechanical and dimensional measurements of the Pulvertaft weave versus the cow-hitch technique. Hand (N Y). 2017; 12:78–84.9. Strandenes E, Ellison P, Mølster A, Gjerdet NR, Moldestad IO, Høl PJ. Strength of Pulvertaft modifications: tensile testing of porcine flexor tendons. J Hand Surg Eur Vol. 2019; 44:795–9.10. Pauchard N, Pedeutour B, Dautel G. [Graft reconstruction of flexor tendons]. Chir Main. 2014; 33 Suppl:S58–71. In French.11. Hashimoto T, Thoreson AR, An KN, Amadio PC, Zhao C. Comparison of step-cut and Pulvertaft attachment for flexor tendon graft: a biomechanics evaluation in an in vitro canine model. J Hand Surg Eur Vol. 2012; 37:848–54.12. Gabuzda GM, Lovallo JL, Nowak MD. Tensile strength of the end-weave flexor tendon repair: an in vitro biomechanical study. J Hand Surg Br. 1994; 19:397–400.13. De Smet L, Schollen W, Degreef I. In vitro biomechanical study to compare the double-loop technique with the Pulvertaft weave for tendon anastomosis. Scand J Plast Reconstr Surg Hand Surg. 2008; 42:305–7.14. Kannan S, Ghosh AI, Dias JJ, Singh HP. Comparative biomechanical characteristics of modified side-to-side repair and modified Pulvertaft weaving repair - in vitro study. J Hand Surg Asian Pac Vol. 2019; 24:76–82.15. Yang C, Zhao C, Amadio PC, Tanaka T, Zhao KD, An KN. Total and intrasynovial work of flexion of human cadaver flexor digitorum profundus tendons after modified Kessler and MGH repair techniques. J Hand Surg Am. 2005; 30:466–70.16. Brown SH, Hentzen ER, Kwan A, Ward SR, Fridén J, Lieber RL. Mechanical strength of the side-to-side versus Pulvertaft weave tendon repair. J Hand Surg Am. 2010; 35:540–5.17. Zhao C, Amadio PC, Momose T, Couvreur P, Zobitz ME, An KN. The effect of suture technique on adhesion formation after flexor tendon repair for partial lacerations in a canine model. J Trauma. 2001; 51:917–21.18. Wu J, Thoreson AR, Reisdorf RL, et al. Biomechanical evaluation of flexor tendon graft with different repair techniques and graft surface modification. J Orthop Res. 2015; 33:731–7.19. Wilbur D, Hammert WC. Principles of tendon transfer. Hand Clin. 2016; 32:283–9.20. Aoki M, Manske PR, Pruitt DL, Kubota H, Larson BJ. Work of flexion after flexor tendon repair according to the placement of sutures. Clin Orthop Relat Res. 1995; (320):205–10.21. Momose T, Amadio PC, Zhao C, Zobitz ME, An KN. The effect of knot location, suture material, and suture size on the gliding resistance of flexor tendons. J Biomed Mater Res. 2000; 53:806–11.22. Amadio PC, Hunter JM, Jaeger SH, Wehbe MA, Schneider LH. The effect of vincular injury on the results of flexor tendon surgery in zone 2. J Hand Surg Am. 1985; 10:626–32.23. Savage R. In vitro studies of a new method of flexor tendon repair. J Hand Surg Br. 1985; 10:135–41.24. Tonkin M, Hagberg L, Lister G, Kutz J. Post-operative management of flexor tendon grafting. J Hand Surg Br. 1988; 13:277–81.25. Vucekovich K, Gallardo G, Fiala K. Rehabilitation after flexor tendon repair, reconstruction, and tenolysis. Hand Clin. 2005; 21:257–65.26. Khan K, Riaz M, Murison MS, Brennen MD. Early active mobilization after second stage flexor tendon grafts. J Hand Surg Br. 1997; 22:372–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative Tensile Load Study of Loop, Interweave, and Kessler Suture Technique using Long Flexor Tendon of Chicken
- Modified Mason-Allen Suture Bridge Technique: A New Suture Bridge Technique with Improved Tissue Holding by the Modified Mason-Allen Stitch
- Modified Pull-out Suture in Posterior Root Tear of the Medial Meniscus: Using a Posteromedial Portal
- Secure and Convenient Three-point and Multi-point Suture Technique
- A Modified Outside-in Suture Technique for Repair of the Middle Segment of the Meniscus Using a Spinal Needle
