Chronic obstructive lung disease after ammonia inhalation burns: a report of two cases
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University Hospital, Busan, Korea
- 2Department of Pathology, Dong-A University Hospital, Busan, Korea
- KMID: 2538865
- DOI: http://doi.org/10.7180/kmj.22.004
Abstract
- Anhydrous ammonia is a commonly used chemical in industry. Ammonia gas inhalation causes thermal injuries and alkali burns in the airway and lung parenchyma. Previous case reports have stated that respiratory sequelae after acute ammonia inhalation burns were associated with structural lung disease, such as bronchiectasis or interstitial lung disease. We herein report two cases of long-term sequelae with persistent airflow limitation after ammonia inhalation burns.
Keyword
Figure
-
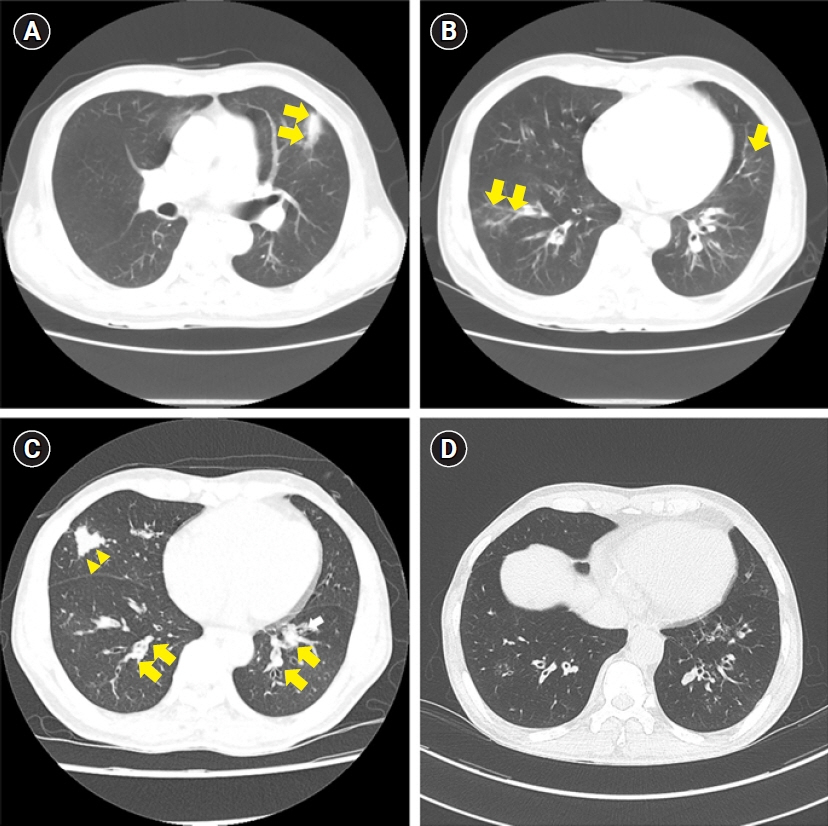
Fig. 1. The chest computed tomography (CT) scan of case 1. (A) The initial chest CT scan with atelectasis (arrows) and (B) patch consolidation (arrows). The follow-up chest CT scan after 6 months with (C) atelectasis (arrowheads) and tubular bronchiectasis with mucus impaction (arrows) (D) after 1 year.
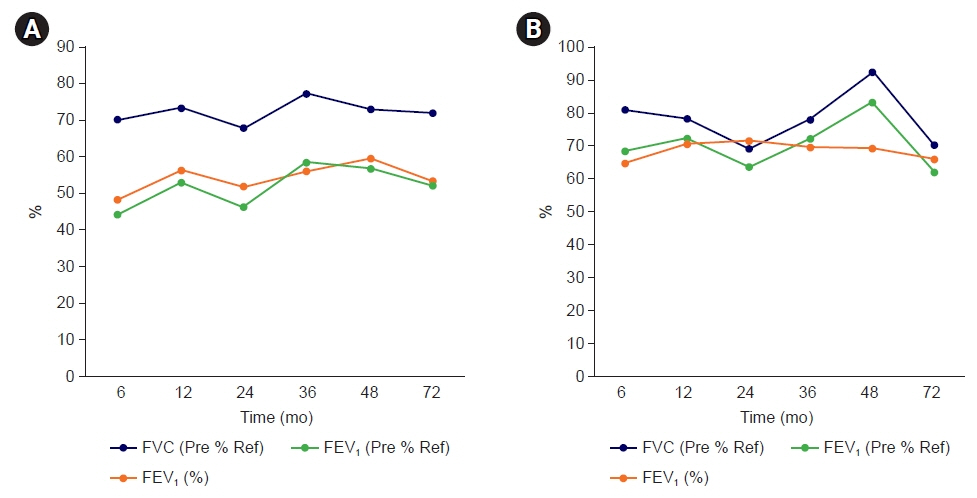
Fig. 2. Serial pulmonary function test results of cases 1 (A) and 2 (B). FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; Ref, reference.
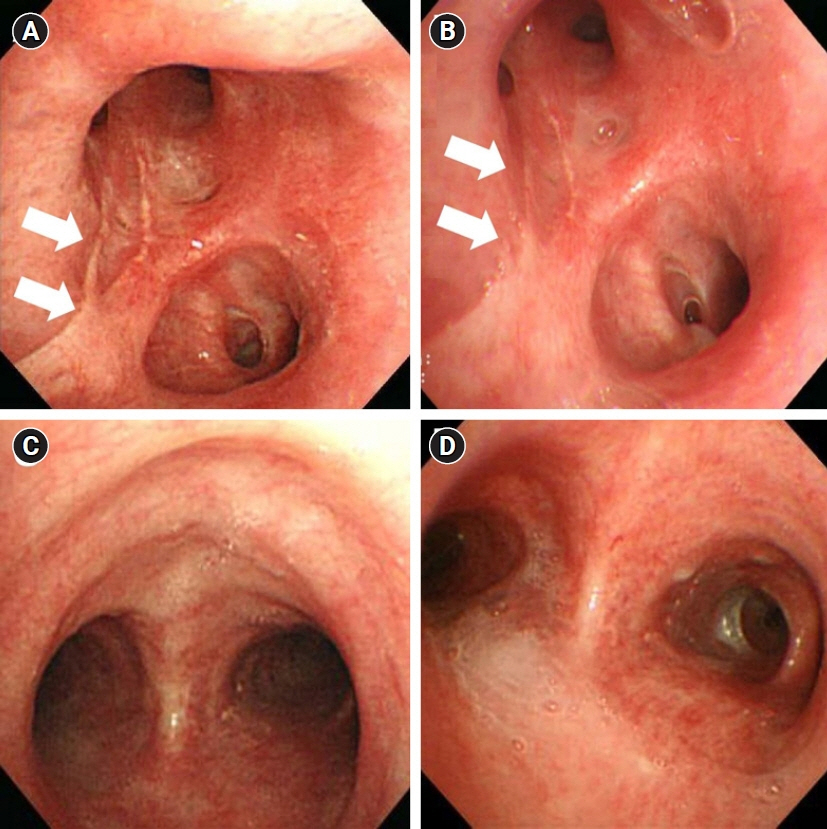
Fig. 3. Bronchoscopy findings of cases 1 and 2. Chemical burn scar changes (arrows) on bronchoscopy performed at 6 months (A) and at 36 months (B) after exposure in case 1. Bronchoscopy findings at 6 months (C) and at 36 months (D) after exposure in case 2.

Fig. 4. Chest computed tomography (CT) scans and chest X-ray image of case 2. (A) The initial chest CT scan with diffuse ground-glass opacities (arrows) in both lower lobes. (B) The initial chest X-ray. (C) A follow-up chest CT scan after 12 months with multifocal ground-glass opacities and consolidations. (D) A follow-up chest CT scan after 24 months with no other abnormalities.
Reference
-
References
1. Arwood R, Hammond J, Ward GG. Ammonia inhalation. J Trauma. 1985; 25:444–7.
Article2. Tonelli AR, Pham A. Bronchiectasis, a long-term sequela of ammonia inhalation: a case report and review of the literature. Burns. 2009; 35:451–3.
Article3. Zhang F, Zheng XF, Ma B, Fan XM, Wang GY, Xia ZF. Mass chemical casualties: treatment of 41 patients with burns by anhydrous ammonia. Burns. 2015; 41:1360–7.
Article4. Leduc D, Gris P, Lheureux P, Gevenois PA, De Vuyst P, Yernault JC. Acute and long term respiratory damage following inhalation of ammonia. Thorax. 1992; 47:755–7.
Article5. Sobonya R. Fatal anhydrous ammonia inhalation. Hum Pathol. 1977; 8:293–9.
Article6. Brautbar N, Wu MP, Richter ED. Chronic ammonia inhalation and interstitial pulmonary fibrosis: a case report and review of the literature. Arch Environ Health. 2003; 58:592–6.
Article7. de la Hoz RE, Schlueter DP, Rom WN. Chronic lung disease secondary to ammonia inhalation injury: a report on three cases. Am J Ind Med. 1996; 29:209–14.
Article8. Pirjavec A, Kovic I, Lulic I, Zupan Z. Massive anhydrous ammonia injury leading to lung transplantation. J Trauma. 2009; 67:E93–7.
Article9. Jones SW, Williams FN, Cairns BA, Cartotto R. Inhalation injury: pathophysiology, diagnosis, and treatment. Clin Plast Surg. 2017; 44:505–11.10. Cha SI, Kim CH, Lee JH, Park JY, Jung TH, Choi WI, et al. Isolated smoke inhalation injuries: acute respiratory dysfunction, clinical outcomes, and short-term evolution of pulmonary functions with the effects of steroids. Burns. 2007; 33:200–8.
Article11. Whitener DR, Whitener LM, Robertson KJ, Baxter CR, Pierce AK. Pulmonary function measurements in patients with thermal injury and smoke inhalation. Am Rev Respir Dis. 1980; 122:731–9.
Article12. Fogarty PW, George PJ, Solomon M, Spiro SG, Armstrong RF. Long term effects of smoke inhalation in survivors of the King’s Cross underground station fire. Thorax. 1991; 46:914–8.
Article13. Moran-Mendoza O, Perez-Padilla JR, Salazar-Flores M, Vazquez-Alfaro F. Wood smoke-associated lung disease: a clinical, functional, radiological and pathological description. Int J Tuberc Lung Dis. 2008; 12:1092–8.14. Ballal SG, Ali BA, Albar AA, Ahmed HO, al-Hasan AY. Bronchial asthma in two chemical fertilizer producing factories in eastern Saudi Arabia. Int J Tuberc Lung Dis. 1998; 2:330–5.15. Lemire P, Dumas O, Chanoine S, Temam S, Severi G, Boutron-Ruault MC, et al. Domestic exposure to irritant cleaning agents and asthma in women. Environ Int. 2020; 144:106017.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of lung injury caused by ammonia-gas inhalation
- Inhalation medications in chronic airway disease
- Encephalopathy Induced by Ammonia Inhalation: Case Reports
- Significance of Bronchodilator Inhalation Test in Obstructive Ventilatory Disorders
- Complications of Chronic Obstructive Pulmonary Disease (COPD)
