Location of Ulnar Nerve Branches to the Flexor Carpi Ulnaris during Surgery for Cubital Tunnel Syndrome
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 2Department of Neurosurgery, Seoul National University Boramae Hospital, Seoul, Korea
- KMID: 2537852
- DOI: http://doi.org/10.3340/jkns.2022.0128
Abstract
Objective
: Cubital tunnel syndrome, the most common ulnar nerve entrapment neuropathy, is usually managed by simple decompression or anterior transposition. One of the concerns in transposition is damage to the nerve branches around the elbow. In this study, the location of ulnar nerve branches to the flexor carpi ulnaris (FCU) was assessed during operations for cubital tunnel syndrome to provide information to reduce operation-related complications.
Methods
: A personal series (HJY) of cases operated for cubital tunnel syndrome was reviewed. Cases managed by transposition and location of branches to the FCU were selected for analysis. The function of the branches was confirmed by intraoperative nerve stimulation and the location of the branches was assessed by the distance from the center of medial epicondyle.
Results
: There was a total of 61 cases of cubital tunnel syndrome, among which 31 were treated by transposition. Twenty-one cases with information on the location of branches were analyzed. The average number of ulnar nerve branches around the elbow was 1.8 (0 to 3), only one case showed no branches. Most of the cases had one branch to the medial head, and one other to the lateral head of the FCU. There were two cases having branches without FCU responses (one branch in one case, three branches in another). The location of the branches to the medial head was 16.3±8.6 mm distal to the medial epicondyle (16 branches; range, 0 to 35 mm), to the lateral head was 19.5±9.5 mm distal to the medial epicondyle (19 branches; range, -5 to 30 mm). Branches without FCU responses were found from 20 mm proximal to the medial condyle to 15 mm distal to the medial epicondyle (five branches). Most of the branches to the medial head were 15 to 20 mm (50% of cases), and most to the lateral head were 15 to 25 mm (58% of cases). There were no cases of discernable weakness of the FCU after operation.
Conclusion
: In most cases of cubital tunnel syndrome, there are ulnar nerve branches around the elbow. Although there might be some cases with branches without FCU responses, most branches are to the FCU, and are to be saved. The operator should be watchful for branches about 15 to 25 mm distal to the medial epicondyle, where most branches come out.
Figure
-
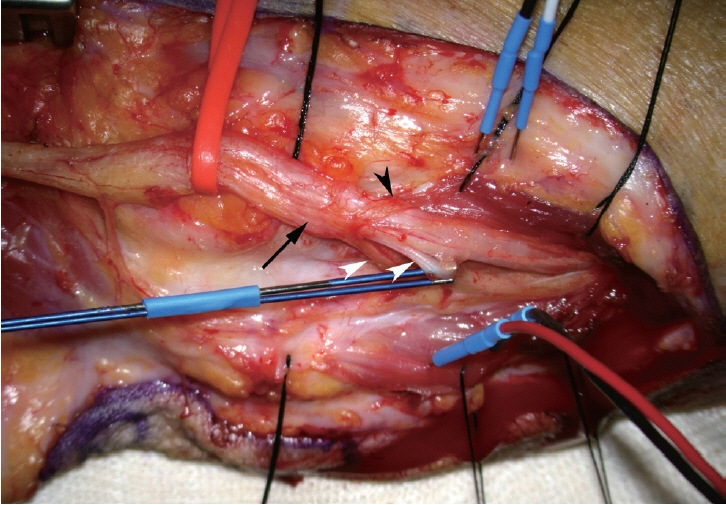
Fig. 1. Photograph showing a common branch to the flexor carpi ulnaris (FCU) from the ulnar nerve taken during anterior transposition of the ulnar nerve left arm. A common branch emerges from the main trunk of the ulnar nerve (black arrow) and then splits into two branches to the medial head of the FCU (white arrowheads) and one branch to the lateral head of the FCU (black arrowhead). The left side of figure is the proximal side of the arm, and the upper side is the anterior side of the arm.
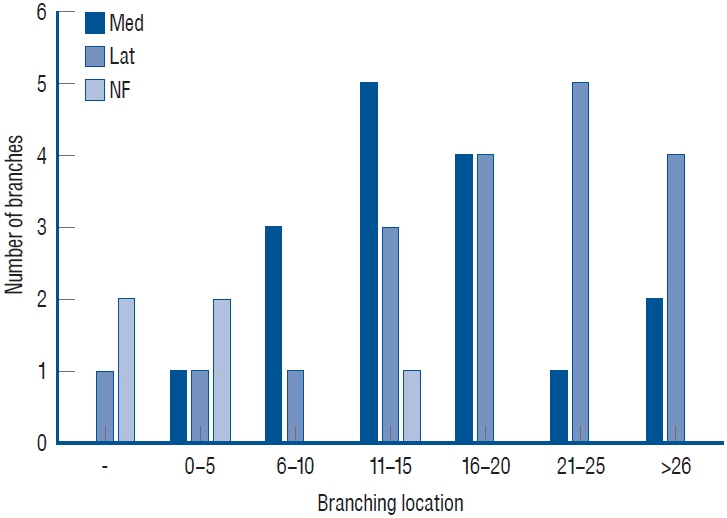
Fig. 2. Location of branches measured from the medial epicondyle. The numbers on the horizontal axis are the distance from the medial epicondyle in millimeters (a negative number means proximal location) and the vertical axis represents the number of medial, lateral, and branches without flexor carpi ulnaris (FCU) responses. More proximal locations are associated with branches without FCU responses (NF), with successively more distal locations for the by medial heads of the flexor carpi ulnaris (Med) and lateral heads (Lat).
Reference
-
References
1. Doyle JR. Surgical Anatomy of the Hand and Upper Extremity. Philadelphia: Lippincott Williams & Wilkins;2003. p204.2. Dugan SH, Lundgren M, Inouye S, Molen JV, Freemyer-Brown A. Variation in the origin of the first motor branch of the ulnar nerve to the flexor carpi ulnaris muscle. FASEB J. 34(S1):1. 2020.3. Marur T, Akkin SM, Alp M, Demirci S, Yalçin L, Ogüt T, et al. The muscular branching patterns of the ulnar nerve to the flexor carpi ulnaris and flexor digitorum profundus muscles. Surg Radiol Anat. 27:322–326. 2005.4. Ogata K, Manske PR, Lesker PA. The effect of surgical dissection on regional blood flow to the ulnar nerve in the cubital tunnel. Clin Orthop Relat Res. (193):195–198. 1985.5. Palmer BA, Hughes TB. Cubital tunnel syndrome. J Hand Surg Am. 35:153–163. 2010.6. Park IJ, Kim HM, Lee JY, Jeong C, Kang Y, Hwang S, et al. Cubital tunnel syndrome caused by anconeus epitrochlearis muscle. J Korean Neurosurg Soc. 61:618–624. 2018.7. Paulos R, Leclercq C. Motor branches of the ulnar nerve to the forearm: an anatomical study and guidelines for selective neurectomy. Surg Radiol Anat. 37:1043–1048. 2015.8. Tubbs RS, Custis JW, Salter EG, Blount JP, Oakes WJ, Wellons JC 3rd. Quantitation of and landmarks for the muscular branches of the ulnar nerve to the forearm for application in peripheral nerve neurotization procedures. J Neurosurg. 104:800–803. 2006.9. Watchmaker GP, Lee G, Mackinnon SE. Intraneural topography of the ulnar nerve in the cubital tunnel facilitates anterior transposition. J Hand Surg Am. 19:915–922. 1994.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Cubital Tunnel Syndrome due to Deep Flexor Pronator Aponeurosis
- Ulnar nerve Compression Syndrome due to anomalous Branch of the Ulnar Nerve Piercing the Flexor Carpi Ulnaris: Report of one case
- Cubital Tunnel Syndrome Caused by Ulnar Nerve Schwannoma: A Case Report
- Cubital Tunnel Syndrome Caused by Osteochondroma: A Case Report
- Ulnar neuropathy
