Hemiballism, a rare complication of coil embilization
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Gumi Hospital, Gumi, Korea
- KMID: 2537321
- DOI: http://doi.org/10.7461/jcen.2022.E2021.07.011
Abstract
- Thromboembolism is one of the major complications during coil embolization of an aneurysm, which usually causes familiar neurological deficits, such as, weakness, aphasia, etc. We report a rare complication by thromboembolism after coil embolization causing hemiballism. A 69-year-old female presented with unruptured posterior communicating artery aneurysm and was treated by coil embolization. After the procedure, the patient showed global aphasia and right hemiparesis, and there were small multiple, scattered infarctions on the left middle cerebral artery territory. The neurologic deficit subsided after five days, but hemballism occurred thereafter. There was no other medical history to explain the hemiballism. The patient was treated with clonazepam and antiepileptics and the hemiballism subsided at postoperative day 20. We report a case of rare complication, hemiballism, during coil embolization.
Figure
-

Fig. 1. Brain computed tomography angiography showing unruptured aneurysms on (A) right paraclinoid carotid artery (arrow), left middle cerebral artery bifurcation (arrowhead), left posterior communicating artery (*), (B) two unruptured aneurysms on right middle cerebral artery (arrow).
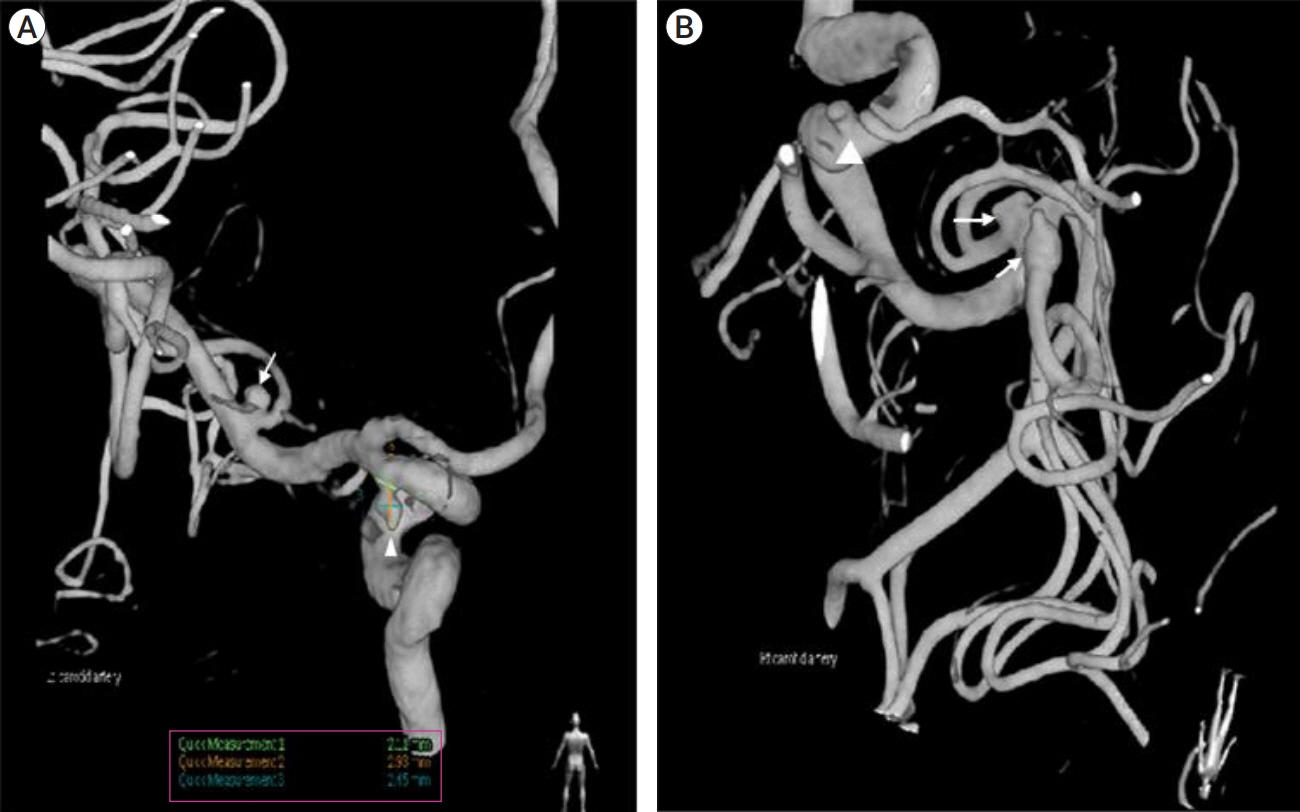
Fig. 2. (A) Left internal carotid artery selection angiogram showing left middle cerebral artery bifurcation unruptured aneurysm (arrow) and left posterior communicating artery unruptured aneurysm (arrowhead). The sizes of the aneurysms are small but the left posterior communicating artery unruptured aneurysm has an irregular shape. (B) Right internal carotid artery selection angiogram showing two unruptured right middle cerebral artery aneurysms (arrow) and right paraclinoid unruptured aneurysm (arrowhead). The sizes of aneurysms are small, but one of the right middle cerebral artery unruptured aneurysm has a bleb on the dome (*).
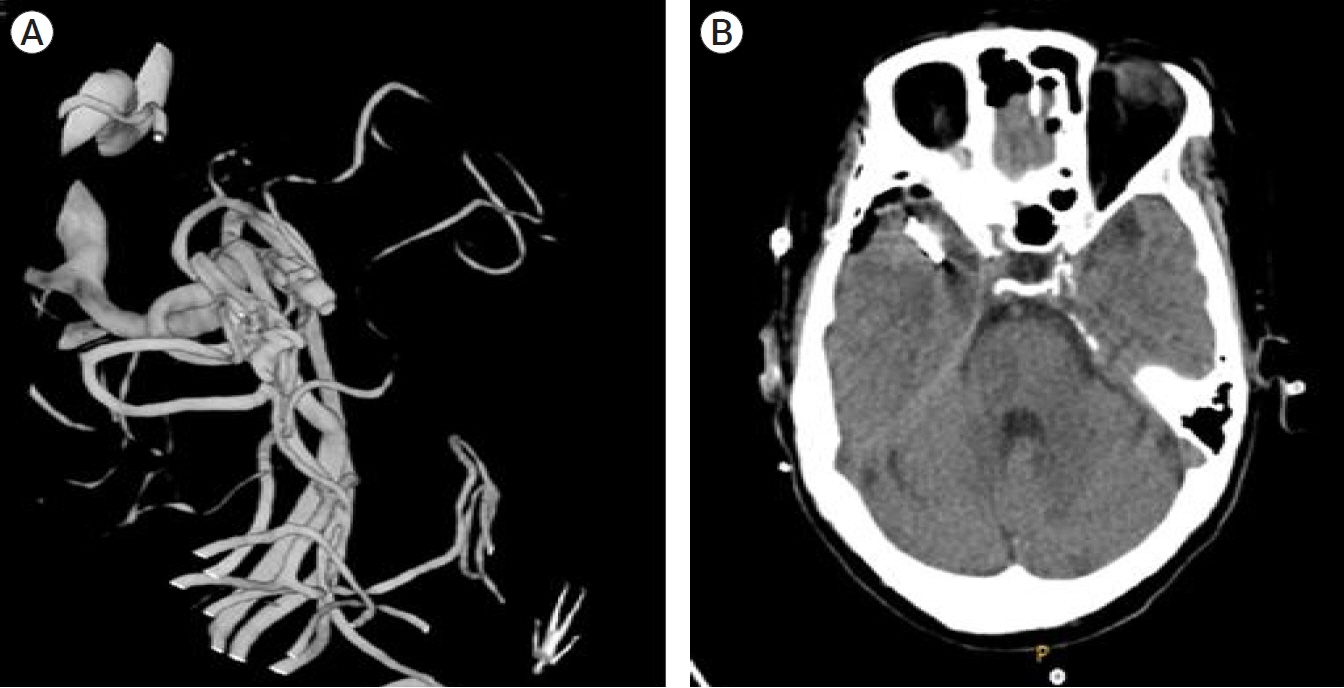
Fig. 3. Postoperative (A) conventional angiogram and (B) brain computed tomogram after aneurysmal neck clipping of the two right middle cerebral artery unruptured aneurysms.
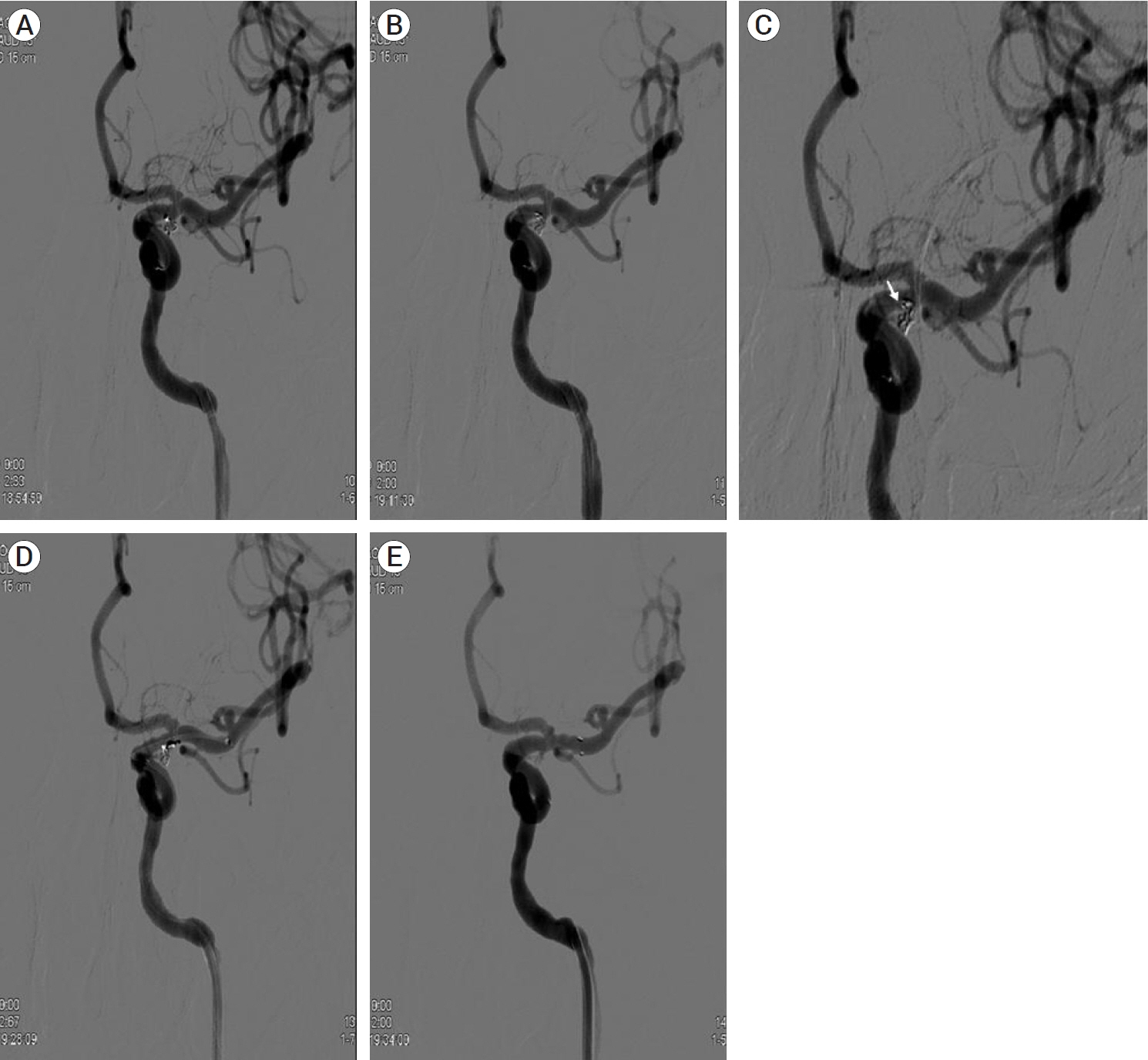
Fig. 4. Coil embolization of left posterior communicating artery aneurysm. (A, B) Framing coil and one additional coil are packed successively. (C) On proceeding coil packing, the microcatheter was unstable and dislodged from the aneurysm and a loop of a coil, which was deployed inside the aneurysm, herniated to the parent artery (arrow). (D, E) To stabilize the herniated loop of coil, a stent is deployed, and the herniated loop of coil is stabilized to the arterial wall by the stent.
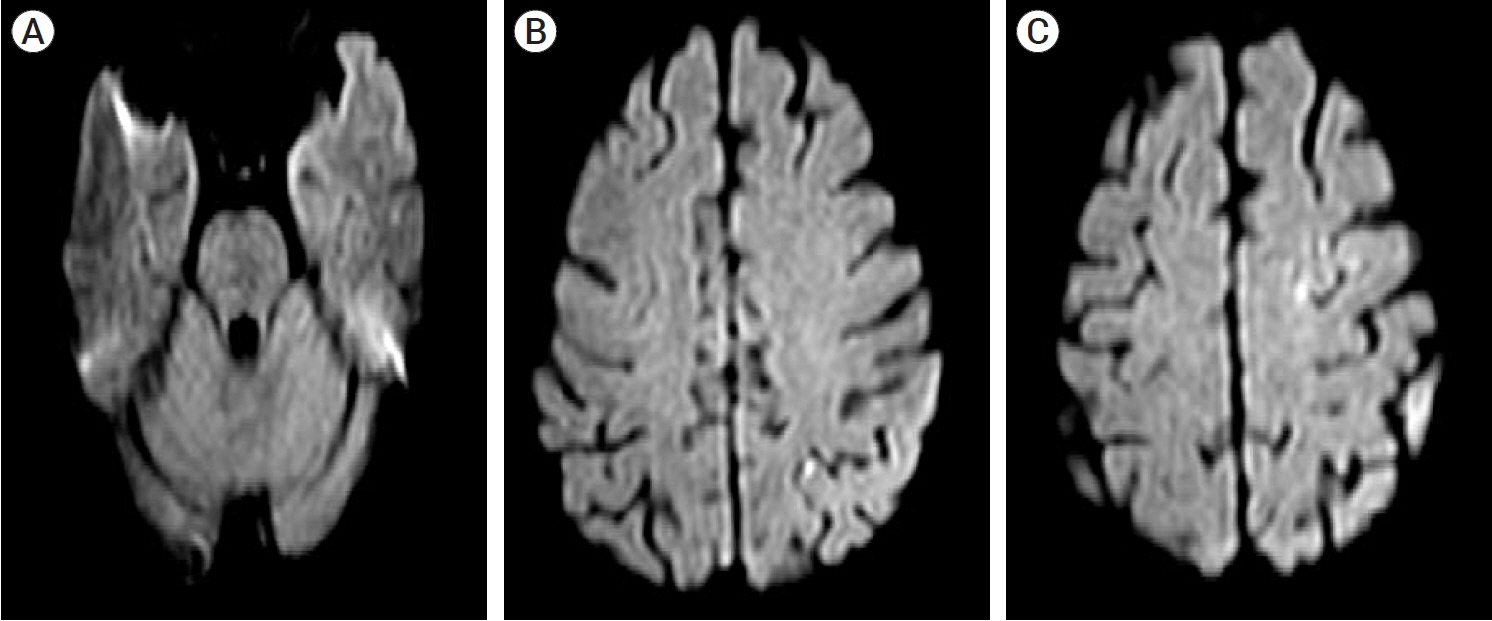
Fig. 5. (A-C) Post-operative diffusion MRI. Diffusion MRI showing small, multiple scattered infarctions on the left frontal, temporal, and parietal cortices, supposedly due to microemboli during the procedure. MRI, magnetic resonance imaging

Fig. 6. The cortico-striato-pallido-thalamo-cortical feedback loop. Thalamus activates the cortex, and interruption in the cortico-striato-pallido-thalamo-cortical feedback loop leading to disinhibition of the thalamus, results in excessive movement, a hyperkinetic movement disorder. Filled arrows indicate inhibitory connections and open arrows indicate excitatory connections. D1, D1 dopamine receptor; D2, D2 dopamine receptor; indirect, indirect pathway; direct, direct pathway; SNc, substantia nigra pars compacta; GPe, external segments of the globus pallidus; STN, subthalamic nucleus; GPi, internal segments of the globus pallidus; SNr, substantia nigra pars reticulata
Reference
-
1. Chung SJ, Im JH, Lee MC, Kim JS. Hemichorea after stroke: clinical-radiological correlation. J Neurol. 2004; Jun. 251(6):725–9.
Article2. Ghika-Schmid F, Ghika J, Regli F, Bogousslavsky J. Hyperkinetic movement disorders during and after acute stroke: the Lausanne Stroke Registry. J Neurol Sci. 1997; Mar. 146(2):109–16.
Article3. Morigaki R, Uno M, Matsubara S, Satoh K, Nagahiro S. Choreoathetosis due to rupture of a distal accessory anterior cerebral artery aneurysm. Cerebrovasc Dis. 2008; 25(3):285–7.
Article4. Morigaki R, Uno M, Suzue A, Nagahiro S. Hemichorea due to hemodynamic ischemia associated with extracranial carotid artery stenosis. Report of two cases. J Neurosurg. 2006; Jul. 105(1):142–7.5. Sakai K, Kyoshima K, Ohigashi Y, Unoki T, Kobayashi S, Meguro M. Generalized choreic movement associated with subarachnoid hemorrhage. No To Shinkei. 1991; 43(9):875–80.6. Scott BL, Jankovic J. Delayed-onset progressive movement disorders after static brain lesions. Neurology. 1996; Jan. 46(1):68–74.
Article7. Shrestha P, Adhikari J, Poudel D, Pathak R, Karmacharya P. Cortical hemiballism: a case of hemiballismus associated with parietal lobe infarct. N Am J Med Sci. 2015; Dec. 7(12):572–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hemiballism as First Isolated Manifestation Following Caudate Infarction
- A Case of Hemiballism in Elderly Stroke Improved by Conventional Rehabilitation Therapy and Low Dose Quetiapine
- Migrated coil and damaged stent removal during coil embolization, using an additional, retrievable stent: A case report
- A Case of Hemiballism-Hemichorea Movement Disorder
- A Case of Hemiballism
