Giant Cardiac Rhabdomyoma with Mixed Atrial Tachycardia and Nonsustained Ventricular Tachycardia in a Newborn with Tuberous Sclerosis
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University Mokdong Hospital, Seoul, Korea
- KMID: 2532211
- DOI: http://doi.org/10.12771/emj.2022.e5
Abstract
- Cardiac rhabdomyomas are typically presented in the tuberous sclerosis. Although benign and often associated with spontaneous regression, in rare circumstances huge mass size and critical location can lead to heart failure, ventricular outflow tract obstruction and refractory tachyarrhythmias. An 1-day-old girl was diagnosed as cardiac tumor during perinatal period. At birth, transthoracic echocardiography revealed huge cardiac mass located in septal area of both ventricle measuring 34×30 mm. It protruded into the left ventricular (LV) outflow tract, potentially obstructing it. A surface ECG revealed atrial tachycardia with nonsustained ventricular tachycardia with heart rate of 217 beats per min. The tachyarrhythmias were controlled with intravenous amiodarone. Reduction of the giant cardiac mass was treated with mammalian target of rapamycin pathway inhibitor sirolimus. However, she unfortunately died at 10 days-old because of sudden cardiac arrest maybe due to LV outflow tract obstruction during therapy. Gene analysis revealed TSC2 mutation after death. (Ewha Med J 2022;45(3):e5)
Figure
-
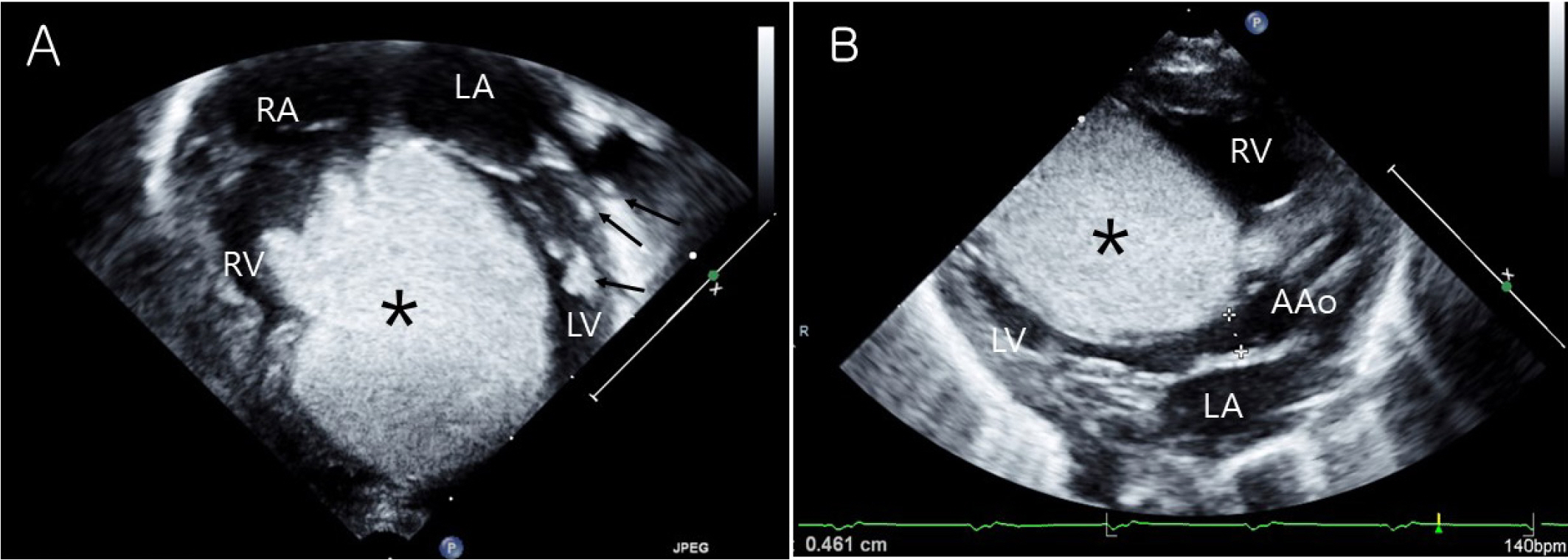
Fig. 1. Transthoracic echocardiography of rhabdomyoma. (A) Huge cardiac mass (asterisks) located in both ventricle measuring 34×30 mm on apical four chamber view. Small multiple cardiac masses (arrows) were located in papillary muscle and chordae tendinae of LV. (B) Cardiac mass (asterisks) protruded into the left ventricular (LV) outflow tract, potentially LV outflow tract obstruction on parasternal long axis view. RV, right ventricle; RA, right atrium; LA, left atrium; LV, left ventricle; AAo, ascending aorta.
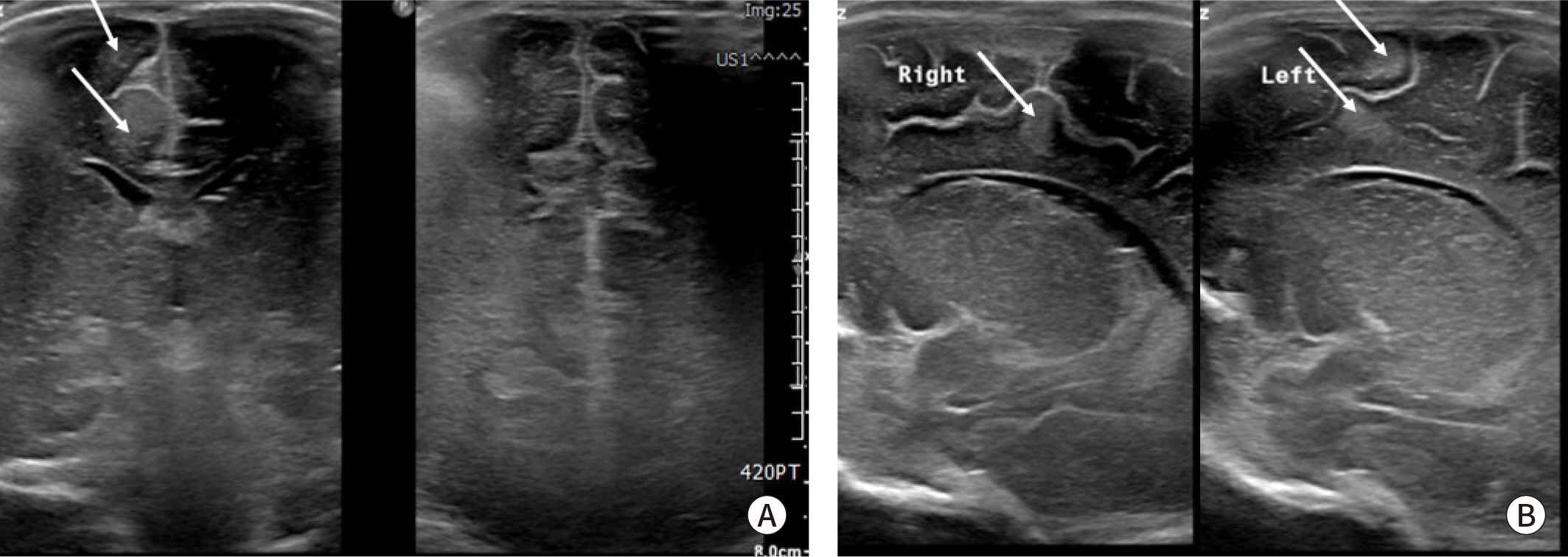
Fig. 2. Brain ultrasound image in neonate with tuberous sclerosis. Multiple cortical and subcortical tuber (arrows) in fronto-parieto-occipital area are showed in (A) coronal view and (B) parasagittal view of right and left brain.
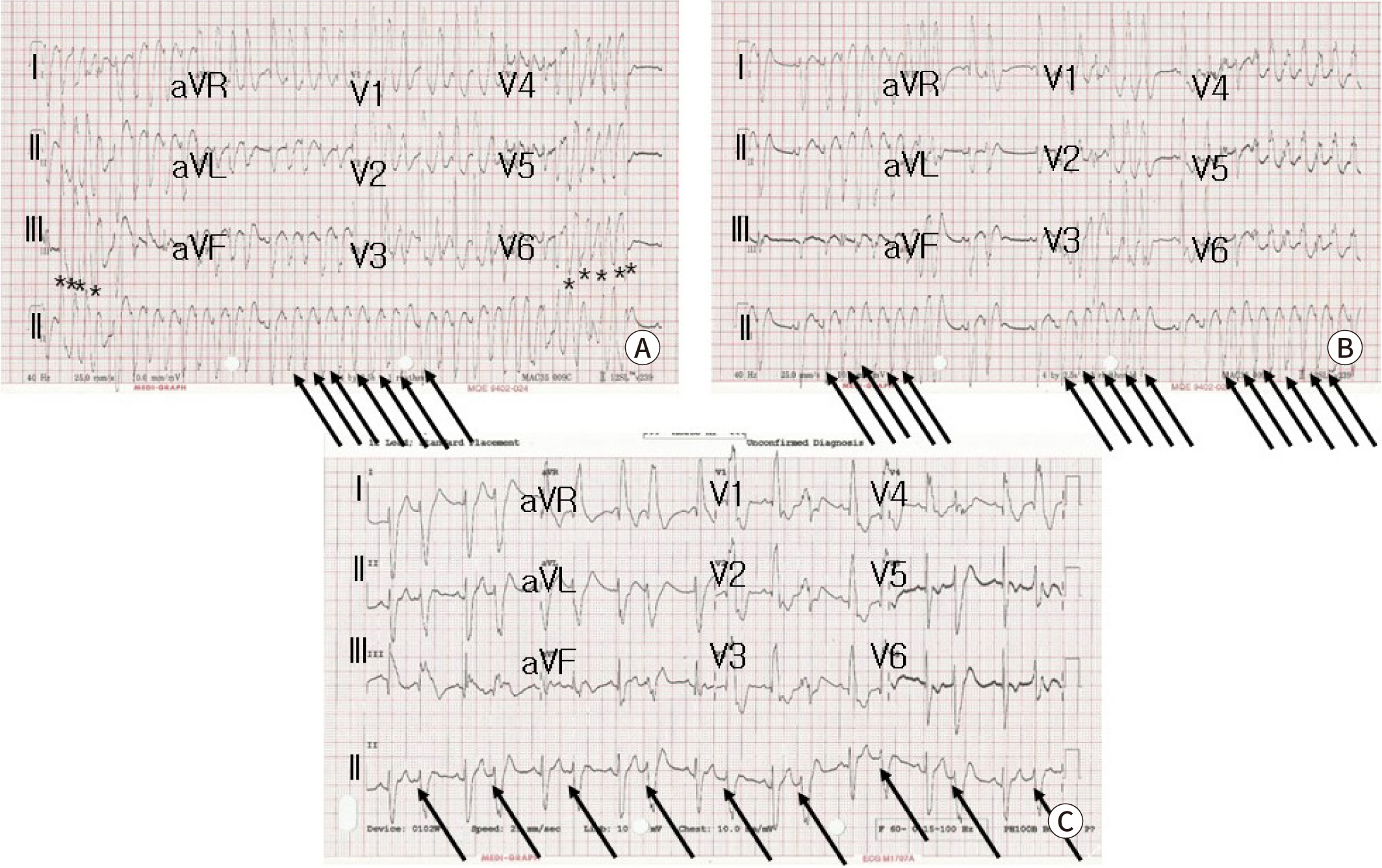
Fig. 3. 12 leads surface ECG showing wide QRS tachycardia. (A) Initial ECG shows atrial tachycardia (arrows) with nonsustained ventriculat tachycardia (asterisks). (B) After amiodarone infusion, nonsustained atrial tachycardia (arrows) and (C) frequent atial premature complex with bigeminy (arrows) are shown.
Reference
-
References
1. Sciacca P, Giacchi V, Mattia C, Greco F, Smilari P, Betta P, et al. Rhabdomyomas and tuberous sclerosis complex: our experience in 33 cases. BMC Cardiovasc Disord. 2014; 14:66. DOI: 10.1186/1471-2261-14-66. PMID: 24884933. PMCID: PMC4039990.
Article2. Verhaaren HA, Vanakker O, De Wolf D, Suys B, François K, Matthys D. Left ventricular outflow obstruction in rhabdomyoma of infancy: meta-analysis of the literature. J Pediatr. 2003; 143:258–263. DOI: 10.1067/S0022-3476(03)00250-6.
Article3. Kwiatkowska J, Wałdoch A, Meyer-Szary J, Potaż P, Grzybiak M. Cardiac tumors in children: a 20-year review of clinical presentation, diagnostics and treatment. Adv Clin Exp Med. 2017; 26:319–326. DOI: 10.17219/acem/62121. PMID: 28791852.
Article4. Dhulipudi B, Bhakru S, Rajan S, Doraiswamy V, Koneti NR. Symptomatic improvement using everolimus in infants with cardiac rhabdomyoma. Ann Pediatr Cardiol. 2019; 12:45–48. DOI: 10.4103/apc.APC_79_18. PMID: 30745769. PMCID: PMC6343372.
Article5. Castro-Monsalve J, Alvarado-Socarras JL, Mantilla KA, Forero L, Moreno A, Prada CE. Cardiac rhabdomyomas in tuberous sclerosis complex. J Pediatr. 2018; 192:264–264.e1. DOI: 10.1016/j.jpeds.2017.09.050. PMID: 29128117.
Article6. Martínez-García A, Michel-Macías C, Cordero-González G, Escamilla-Sánchez KI, Aguinaga-Ríos M, Coronado-Zarco A, et al. Giant left ventricular rhabdomyoma treated successfully with everolimus: case report and review of literature. Cardiol Young. 2018; 28:903–909. DOI: 10.1017/S1047951118000598. PMID: 29759095.
Article7. Ninic S, Kalaba M, Jovicic B, Vukomanovic V, Prijic S, Vucetic B, et al. Successful use of sirolimus for refractory atrial ectopic tachycardia in a child with cardiac rhabdomyoma. Ann Noninvasive Electrocardiol. 2017; 22:e12435. DOI: 10.1111/anec.12435. PMID: 28217909. PMCID: PMC6931800.
Article8. Kathare PA, Muthuswamy KS, Sadasivan J, Calumbar N, Koneti NR. Incessant ventricular tachycardia due to multiple cardiac rhabdomyomas in an infant with tuberous sclerosis. Indian Heart J. 2013; 65:111–113. DOI: 10.1016/j.ihj.2012.12.003. PMID: 23438626. PMCID: PMC3860908.
Article9. Wacker-Gussmann A, Strasburger JF, Cuneo BF, Wiggins DL, Gotteiner NL, Wakai RT. Fetal arrhythmias associated with cardiac rhabdomyomas. Heart Rhythm. 2014; 11:677–683. DOI: 10.1016/j.hrthm.2013.12.018. PMID: 24333285. PMCID: PMC3965621.
Article10. Öztunç F, Atik SU, Güneş AO. Everolimus treatment of a newborn with rhabdomyoma causing severe arrhythmia. Cardiol Young. 2015; 25:1411–1414. DOI: 10.1017/S1047951114002261. PMID: 26339757.
Article11. Brugada J, Blom N, Sarquella-Brugada G, Blomstrom-Lundqvist C, Deanfield J, Janousek J, et al. Pharmacological and non-pharmacological therapy for arrhythmias in the pediatric population: EHRA and AEPC-Arrhythmia Working Group joint consensus statement. Europace. 2013; 15:1337–1382. DOI: 10.1093/europace/eut082. PMID: 23851511.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Response to Letter to the Editor: Giant Cardiac Rhabdomyoma with Mixed Atrial Tachycardia and Nonsustained Ventricular Tachycardia in a Newborn with Tuberous Sclerosis
- Letter to the Editor: Giant Cardiac Rhabdomyoma with Mixed Atrial Tachycardia and Nonsustained Ventricular Tachycardia in a Newborn with Tuberous Sclerosis
- A Case of Repeated Ventricular Tachycardia Caused by Cardiac Rhabdomyomas in an Infant with Tuberous Sclerosis
- Supraventricular tachycardia in a neonate with cardiac rhabdomyoma and tuberous sclerosis
- Multiple Rhabomyomas in left Ventricular Outflow Tract Combined with Tuberous Sclerosis: A Case Report
