Two cases of late-onset cardiovascular toxicities after a single injection of local anesthetics during supraclavicular brachial plexus block - A report of two cases -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Inje University Ilsan Paik Hospital, Goyang, Korea
- KMID: 2531700
- DOI: http://doi.org/10.17085/apm.21093
Abstract
- Background
Local anesthetics systemic toxicity (LAST) is a grave complication of regional anesthesia that usually occurs immediately after local anesthetics injection. Here, we report on rare late-onset toxicity cases after supraclavicular brachial plexus blocks. Case: Two patients underwent surgery for radius fractures. We used lidocaine 100 mg and ropivacaine 150 mg for blocking and infused dexmedetomidine for intraoperative sedation. The 63-year-old male patient’s blood pressure dropped to 87/60 mmHg after 3 h 15 min after blocking. Ventricular fibrillation occurred 10 min later. After five defibrillations, electrocardiography showed ventricular tachycardia that was normalized through one cardioversion. The 54-year-old female patient’s heart rate decreased to 35 beats/min 2 h 30 min after blocking. Her vital signs returned to normal after administering atropine, ephedrine, epinephrine, and lipid emulsion. Conclusions: Physicians should remember that LAST may occur long after local anesthetic injection and be aware of factors that may adversely affect the course of LAST.
Figure
-
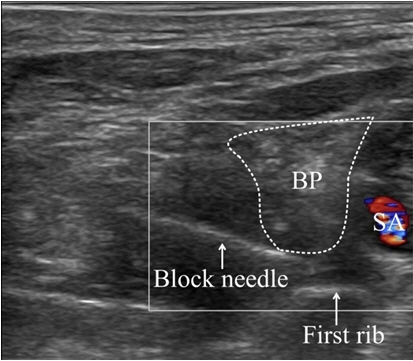
Fig. 1. Ultrasonography image of supraclavicular brachial plexus with color doppler. BP: brachial plexus, SA: subclavian artery.
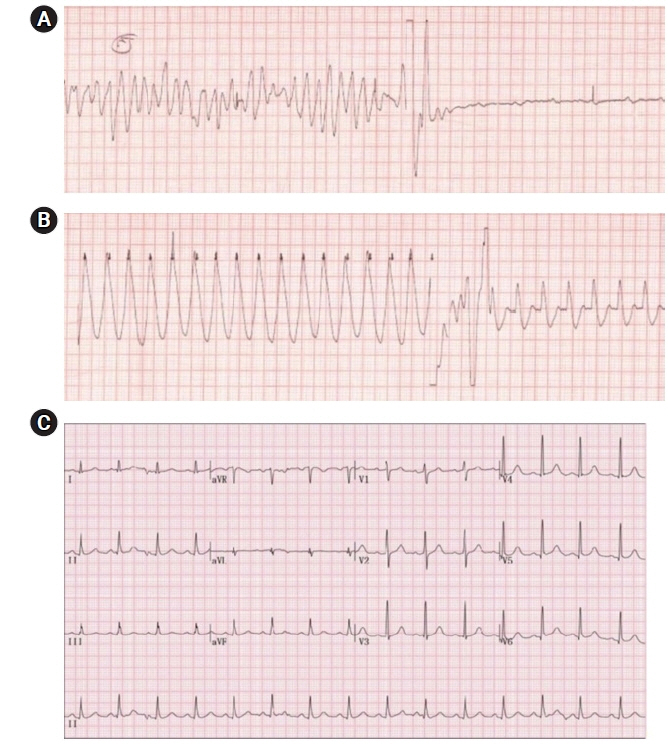
Fig. 2. Electrocardiography of the patient. (A) Ventricular fibrillation. (B) Ventricular tachycardia. (C) QT prolongation: heart rate-corrected QT interval = 484 milliseconds.
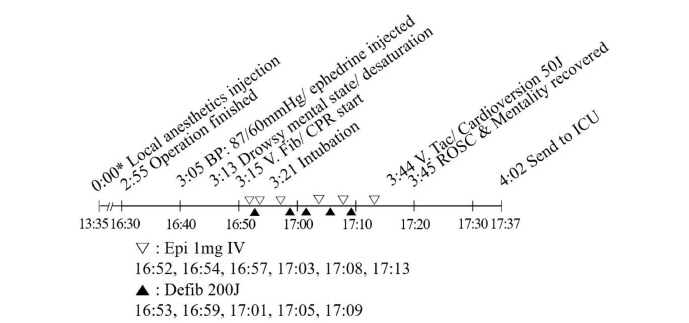
Fig. 3. Timeline of the first case. BP: blood pressure, CPR: cardiopulmonary resuscitation, Defib: defibrillation, Epi: epinephrine, ICU: intensive care unit, IV: intravenously, ROSC: return of spontaneous circulation, V. Fib: ventricular fibrillation, V. Tac: ventricular tachycardia. *Indicates time after the local anesthetics injection.

Fig. 4. Timeline of the second case. HR: heart rate, IV: intravenously, NIBP: non-invasive blood pressure, PACU: post-anesthesia care unit. *Indicates time after the local anesthetics injection.
Reference
-
1. El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. 2018; 11:35–44.
Article2. Macfarlane AJR, Gitman M, Bornstein KJ, El-Boghdadly K, Weinberg G. Updates in our understanding of local anaesthetic systemic toxicity: a narrative review. Anaesthesia. 2021; 76 Suppl 1:27–39.
Article3. Gitman M, Fettiplace MR, Weinberg GL, Neal JM, Barrington MJ. Local anesthetic systemic toxicity: a narrative literature review and clinical update on prevention, diagnosis, and management. Plast Reconstr Surg. 2019; 144:783–95.4. Gitman M, Barrington MJ. Local anesthetic systemic toxicity: a review of recent case reports and registries. Reg Anesth Pain Med. 2018; 43:124–30.5. Oh S, Chung J, Lee SM, Chung K, Kwon K. Late onset of systemic toxicity of local anesthetics in brachial plexus block: a case report. Anesth Pain Med. 2012; 7:372–4.6. İnceöz H, Tutal ZB, Babayiğit M, Kepek A, Horasanlı E. Late local anaesthetic toxicity after infraclavicular block procedure. Turk J Anaesthesiol Reanim. 2015; 43:199–201.
Article7. Lui KC, Chow YF. Safe use of local anaesthetics: prevention and management of systemic toxicity. Hong Kong Med J. 2010; 16:470–5.8. Knudsen K, Beckman Suurküla M, Blomberg S, Sjövall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997; 78:507–14.
Article9. Scott DB, Lee A, Fagan D, Bowler GM, Bloomfield P, Lundh R. Acute toxicity of ropivacaine compared with that of bupivacaine. Anesth Analg. 1989; 69:563–9.
Article10. Sepehripour S, Dheansa BS. Is there an advantage in onset of action with mixing lignocaine and bupivacaine? J Plast Reconstr Aesthet Surg. 2017; 70:1782.
Article11. Cuvillon P, Nouvellon E, Ripart J, Boyer JC, Dehour L, Mahamat A, et al. A comparison of the pharmacodynamics and pharmacokinetics of bupivacaine, ropivacaine (with epinephrine) and their equal volume mixtures with lidocaine used for femoral and sciatic nerve blocks: a double-blind randomized study. Anesth Analg. 2009; 108:641–9.
Article12. Bharati S, Pal A, Biswas C, Biswas R. Incidence of cardiac arrest increases with the indiscriminate use of dexmedetomidine: a case series and review of published case reports. Acta Anaesthesiol Taiwan. 2011; 49:165–7.
Article13. Beloeil H, Garot M, Lebuffe G, Gerbaud A, Bila J, Cuvillon P, et al. POFA Study Group; SFAR Research Network. Balanced opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery: the postoperative and opioid-free anesthesia (POFA) randomized clinical trial. Anesthesiology. 2021; 134:541–51.14. Canbora MK, Polat A, Subaşı FD, Ulkü TK. Carotid sinus hypersensitivity due to shoulder sling pressure after arthroscopic rotator cuff repair: a case report. Acta Orthop Traumatol Turc. 2012; 46:308–11.
Article15. Neal JM, Barrington MJ, Fettiplace MR, Gitman M, Memtsoudis SG, Mörwald EE, et al. The third American Society of Regional Anesthesia and Pain Medicine practice advisory on local anesthetic systemic toxicity: executive summary 2017. Reg Anesth Pain Med. 2018; 43:113–23.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Late onset of systemic toxicity of local anesthetics in brachial plexus block: A case report
- Unilateral Horner's Syndrome following supraclavicular brachial plexus block
- Cases series: ultrasound-guided supraclavicular block in 105 patients
- Clinical Evaluation of Supraclavicular Block ; Influence of Injected Volume of Bupivacaine on Neural Blockade
- The Effect of Fentanyl or Epinephrine Addition to Ropivacaine in Brachial Plexus Block
