Is Age-Predicted Maximal Heart Rate Applicable in Patients With Heart or Lung Disease?
- Affiliations
-
- 1Department of Rehabilitation Medicine and Biomedical Research Institute, Pusan National University Hospital, Busan, Korea
- 2Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea
- KMID: 2531284
- DOI: http://doi.org/10.5535/arm.21181
Abstract
Objective
To compare the predicted and actual maximal heart rate (HRmax) values in the cardiopulmonary exercise test (CPET).
Methods
We retrospectively investigated 1,060 patients who underwent a CPET between January 2016 and April 2020 at our institution’s cardiopulmonary rehabilitation center. The following patients were included: those aged >20 years, those tested with a treadmill, and those who underwent symptom-limited maximum exercise testing— reaching ≥85% of the predicted HRmax (62% if taking beta-blockers) and highest respiratory exchange ratio ≥1.1. Ultimately, 827 patients were included in this study. Data on diagnosis, history of taking beta-blockers, age, body mass index (BMI), and CPET parameters were collected. Subgroup analysis was performed according to age, betablockers, BMI (low <18.5 kg/m2, normal, and high ≥25 kg/m2), and risk classification.
Results
There was a significant difference between the actual HRmax and the predicted value (p<0.001). Betablocker administration resulted in a significant difference in the actual HRmax (p<0.001). There were significant differences in the moderate-to-high-risk and low-risk groups and the normal BMI and high BMI groups (p<0.001). There was no significant difference between the elderly and younger groups. We suggest new formulae for HRmax of cardiopulmonary patients: estimated HRmax=183-0.76×age (the beta-blocker group) and etimated HRmax=210-0.91×age (the non-beta-blocker group).
Conclusion
Age-predicted HRmax was significantly different from the actual HRmax of patients with cardiopulmonary disease, especially in the beta-blocker group. For participants with high BMI and moderate-tosevere risk, the actual HRmax was significantly lower than the predicted HRmax.
Keyword
Figure
-
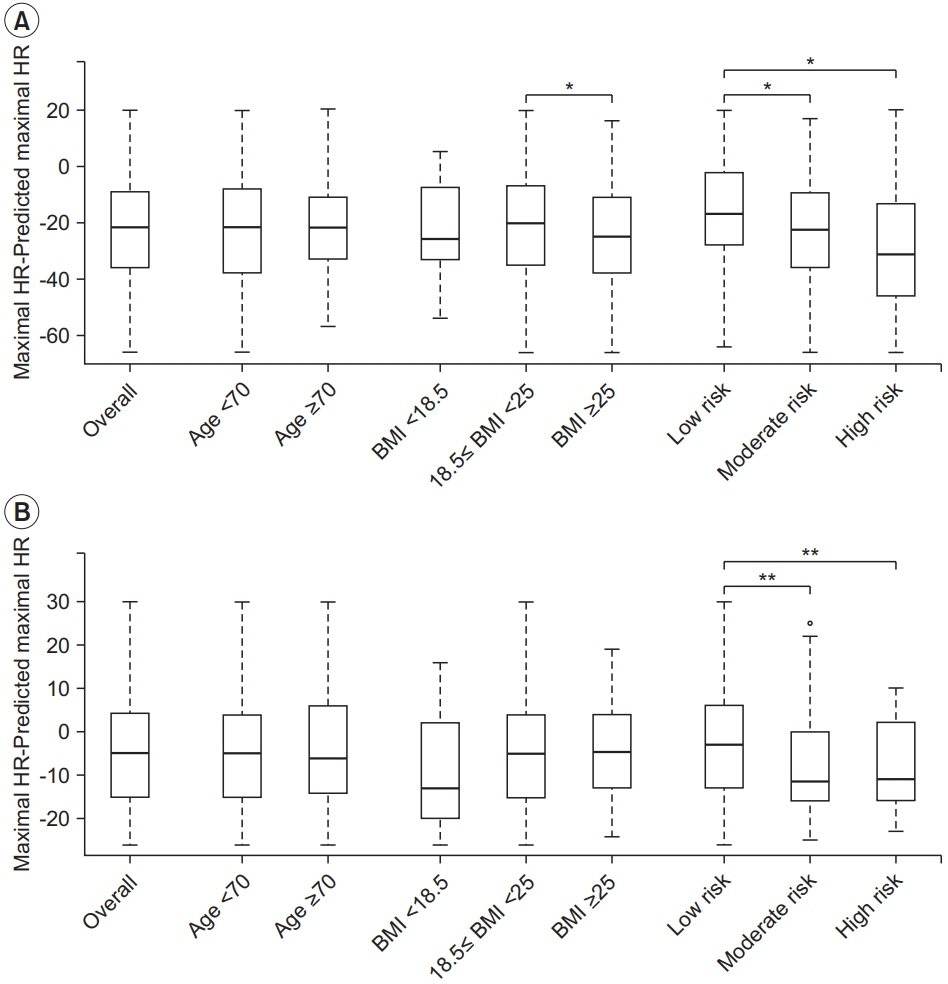
Fig. 1. Comparison of actual maximal heart rate (HR) and age-predicted maximal HR. Boxplots of (A) beta-blocker group (n=431) and (B) non-beta-blocker group (n=431). Participants were divided into subgroups according to age, body mass index (BMI, kg/m2), and risk classification. *p<0.05 (Bonferroni correction for continuous variable), **p<0.05 (least significant difference correction for continuous variable).
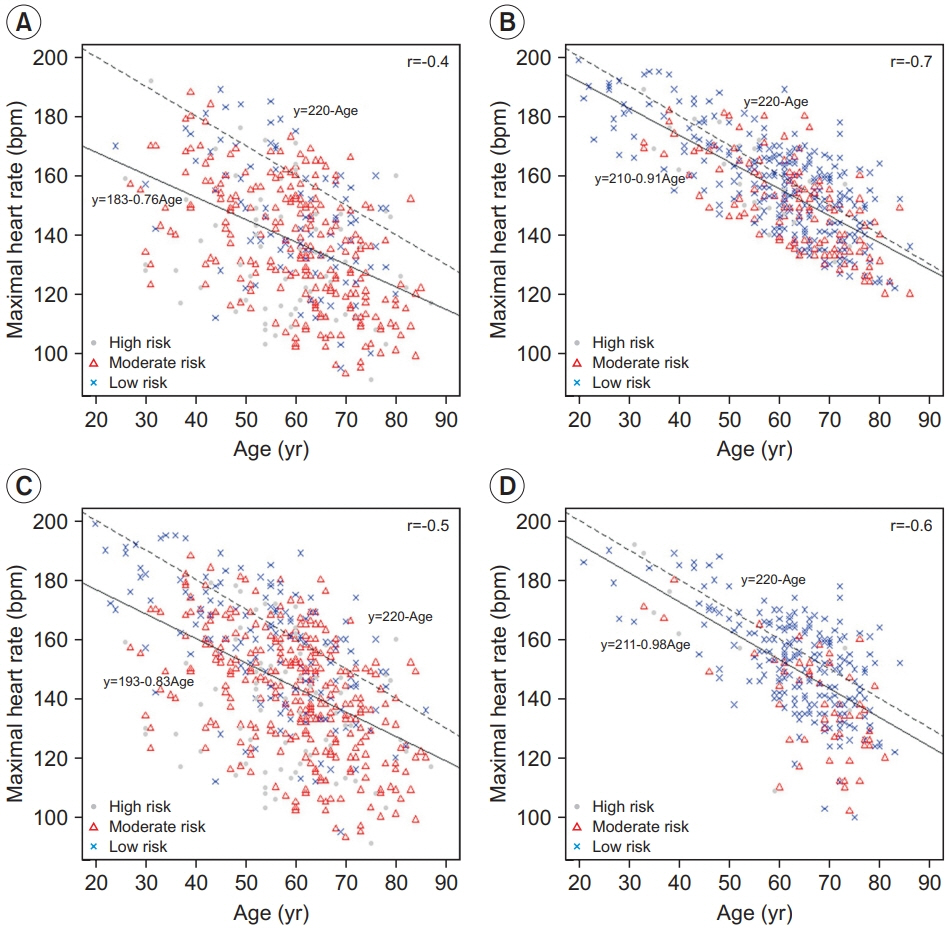
Fig. 2. Scatterplot between age and actual maximal heart rate (n=827). Divided into two groups depending on whether they were taking beta-blockers or not. (A) Group with taking beta-blockers (n=396). (B) Group without betablockers (n=431). And divided into by disease group, (C) cardiac disease group (n=537) and (D) pulmonary disease group (n=290). All participants were classified into high risk, moderate risk, and low risk according to the risk classification and displayed in different diagrams.
Reference
-
1. Karvonen J, Vuorimaa T. Heart rate and exercise intensity during sports activities: practical application. Sports Med. 1988; 5:303–11.2. Esposito F, Impellizzeri FM, Margonato V, Vanni R, Pizzini G, Veicsteinas A. Validity of heart rate as an indicator of aerobic demand during soccer activities in amateur soccer players. Eur J Appl Physiol. 2004; 93:167–72.
Article3. Hills AP, Byrne NM, Ramage AJ. Submaximal markers of exercise intensity. J Sports Sci. 1998; 16 Suppl:S71–6.
Article4. Sebastian LA, Reeder S, Williams M. Determining target heart rate for exercising in a cardiac rehabilitation program: a retrospective study. J Cardiovasc Nurs. 2015; 30:164–71.5. Albouaini K, Egred M, Alahmar A, Wright DJ. Cardiopulmonary exercise testing and its application. Postgrad Med J. 2007; 83:675–82.
Article6. Ozeki N, Fukui T, Iwano S, Hakiri S, Nakamura S, Kawaguchi K, et al. Factors associated with changes in the 12-m stair-climbing time after lung lobectomy. Gen Thorac Cardiovasc Surg. 2021; 69:282–9.
Article7. Fox SM 3rd, Naughton JP, Haskell WL. Physical activity and the prevention of coronary heart disease. Ann Clin Res. 1971; 3:404–32.
Article8. Sporis G, Vucetic V, Jukic I, Omrcen D, Bok D, Custonja Z. How reliable are the equations for predicting maximal heart rate values in military personnel? Mil Med. 2011; 176:347–51.
Article9. Lewis GD, Bossone E, Naeije R, Grunig E, Saggar R, Lancellotti P, et al. Pulmonary vascular hemodynamic response to exercise in cardiopulmonary diseases. Circulation. 2013; 128:1470–9.
Article10. Robergs RA, Landwehr R. The surprising history of the “HRmax=220-age” equation. J Exerc Physiol Online. 2002; 5:1–10.11. Londeree BR, Moeschberger ML. Influence of age and other factors on maximal heart rate. J Cardiac Rehabil. 1984; 4:44–9.12. Miller WC, Wallace JP, Eggert KE. Predicting max HR and the HR-VO2 relationship for exercise prescription in obesity. Med Sci Sports Exerc. 1993; 25:1077–81.13. Strait JB, Lakatta EG. Aging-associated cardiovascular changes and their relationship to heart failure. Heart Fail Clin. 2012; 8:143–64.
Article14. Wonisch M, Hofmann P, Fruhwald FM, Kraxner W, Hodl R, Pokan R, et al. Influence of beta-blocker use on percentage of target heart rate exercise prescription. Eur J Cardiovasc Prev Rehabil. 2003; 10:296–301.
Article15. Kligfield P, Lauer MS. Exercise electrocardiogram testing: beyond the ST segment. Circulation. 2006; 114:2070–82.16. Hong SP, Lee YS, Lee JB, Ryu JK, Choi JY, Kim KS. Prognostic value of heart rate reserve in exercise treadmill test after coronary revascularization. Intern Med. 2014; 4:175.
Article17. Salati M, Brunelli A. Risk stratification in lung resection. Curr Surg Rep. 2016; 4:37.
Article18. Khan SS, Ning H, Wilkins JT, Allen N, Carnethon M, Berry JD, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018; 3:280–7.
Article19. Li S, Wang Z, Huang J, Fan J, Du H, Liu L, et al. Systematic review of prognostic roles of body mass index for patients undergoing lung cancer surgery: does the ‘obesity paradox’ really exist? Eur J Cardiothorac Surg. 2017; 51:817–28.
Article20. Zewari S, Vos P, van den Elshout F, Dekhuijzen R, Heijdra Y. Obesity in COPD: revealed and unrevealed issues. COPD. 2017; 14:663–73.
Article21. Toner MM, Sawka MN, Levine L, Pandolf KB. Cardiorespiratory responses to exercise distributed between the upper and lower body. J Appl Physiol Respir Environ Exerc Physiol. 1983; 54:1403–7.
Article22. Lafortuna CL, Lazzer S, Agosti F, Busti C, Galli R, Mazzilli G, et al. Metabolic responses to submaximal treadmill walking and cycle ergometer pedalling in obese adolescents. Scand J Med Sci Sports. 2010; 20:630–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Heart transplantation in a patient with complex heart lung disease: a case report
- Selection of Aerobic Exercise Intensity Using Heart Rate Reserve in Stroke Patients
- Recent Advancement in Heart and Lung Transplantation
- Changes in Heart Rate during and after Exercise Treadmill Test as Prognostic Factor in Cardiovascular Disease
- The Role of Multistage Maximal Exercise Test in the Evaluation of Patient for Various Heart Disease
