Comparison of Prevailing Insulin Regimens at Different Time Periods in Hospitalized Patients: A Real-World Experience from a Tertiary Hospital
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
- 2Division of Endocrinology and Metabolism, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- KMID: 2530183
- DOI: http://doi.org/10.4093/dmj.2021.0065
Abstract
- Background
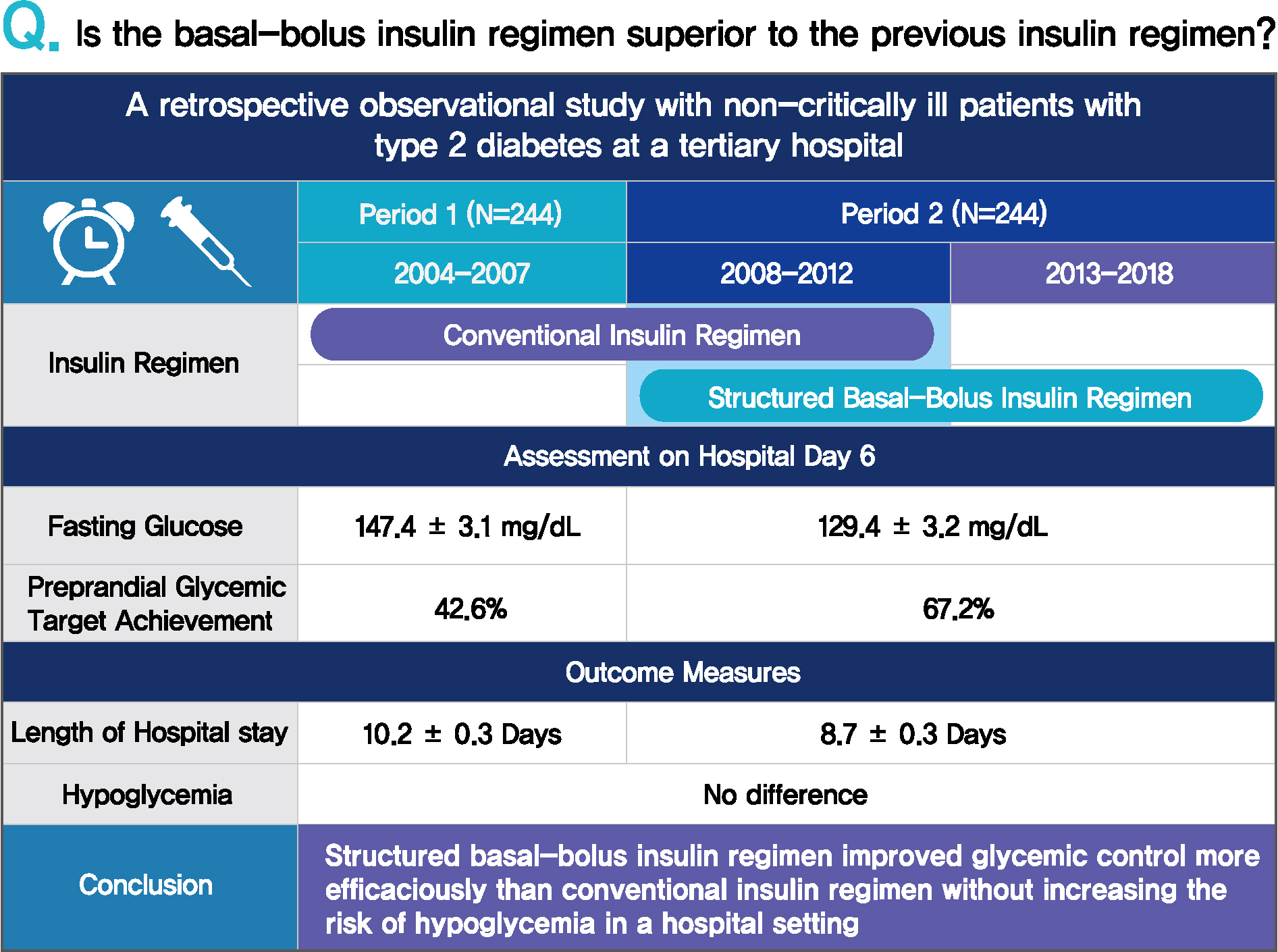
Prevailing insulin regimens for glycemic control in hospitalized patients have changed over time. We aimed to determine whether the current basal-bolus insulin (BBI) regimen is superior to the previous insulin regimen, mainly comprising split-mixed insulin therapy.
Methods
This was a single tertiary center, retrospective observational study that included non-critically ill patients with type 2 diabetes mellitus who were treated with split-mixed insulin regimens from 2004 to 2007 (period 1) and with BBI from 2008 to 2018 (period 2). Patients from each period were analyzed after propensity score matching. The mean difference in glucose levels and the achievement of fasting and preprandial glycemic targets by day 6 of admission were assessed. The total daily insulin dose, incidence of hypoglycemia, and length of hospital stay were also evaluated.
Results
Among 244 patients from each period, both fasting glucose (estimated mean±standard error, 147.4±3.1 mg/dL vs. 129.4±3.2 mg/dL, P<0.001, day 6) and preprandial glucose (177.7±2.8 mg/dL vs. 152.8±2.8 mg/dL, P<0.001, day 6) were lower in period 2 than in period 1. By day 6 of hospital admission, 42.6% and 67.2% of patients achieved a preprandial glycemic target of <140 mg/dL in periods 1 and 2, respectively (relative risk, 2.00; 95% confidence interval, 1.54 to 2.59), without an increased incidence of hypoglycemia. Length of stay was shorter in period 2 (10.23±0.26 days vs. 8.70±0.26 days, P<0.001).
Conclusion
BBI improved glycemic control in a more efficacious manner than a split-mixed insulin regimen without increasing the risk of hypoglycemia in a hospital setting.
Keyword
Figure
-

Fig. 1. Glycemic control during hospital stay. Data shown are the glucose values (estimated mean±standard error) obtained from each time point with 95% confidence intervals. Analysis of covariance (ANCOVA) analyses were performed, adjusted for age, sex, body mass index, weight, estimated glomerular filtration rate, diabetes duration, glycated hemoglobin, number of concurrent antidiabetic medications, the usage frequency of each antidiabetic medication, and the number of plasma glucose measurements by point-of-care testing. (A) Mean glucose from day 1 to 6 according to time of the day. (B) Mean glucose from day 1 to 2 vs. day 5 to 6. (C) Preprandial glucose from day 1 to 6. (D) Fasting glucose from day 2 to 6. (E) Kaplan-Meier analysis of target achievement of the mean preprandial glucose on each day. (F) Kaplan-Meier analysis of target achievement of all preprandial (i.e., pre-breakfast, pre-lunch, and pre-dinner) glucose on each day. aP<0.05 for period 1 day 1 to 2 vs. period 2 day 1 to 2, bP<0.05 for period 1 day 5 to 6 vs. period 2 day 5 to 6.
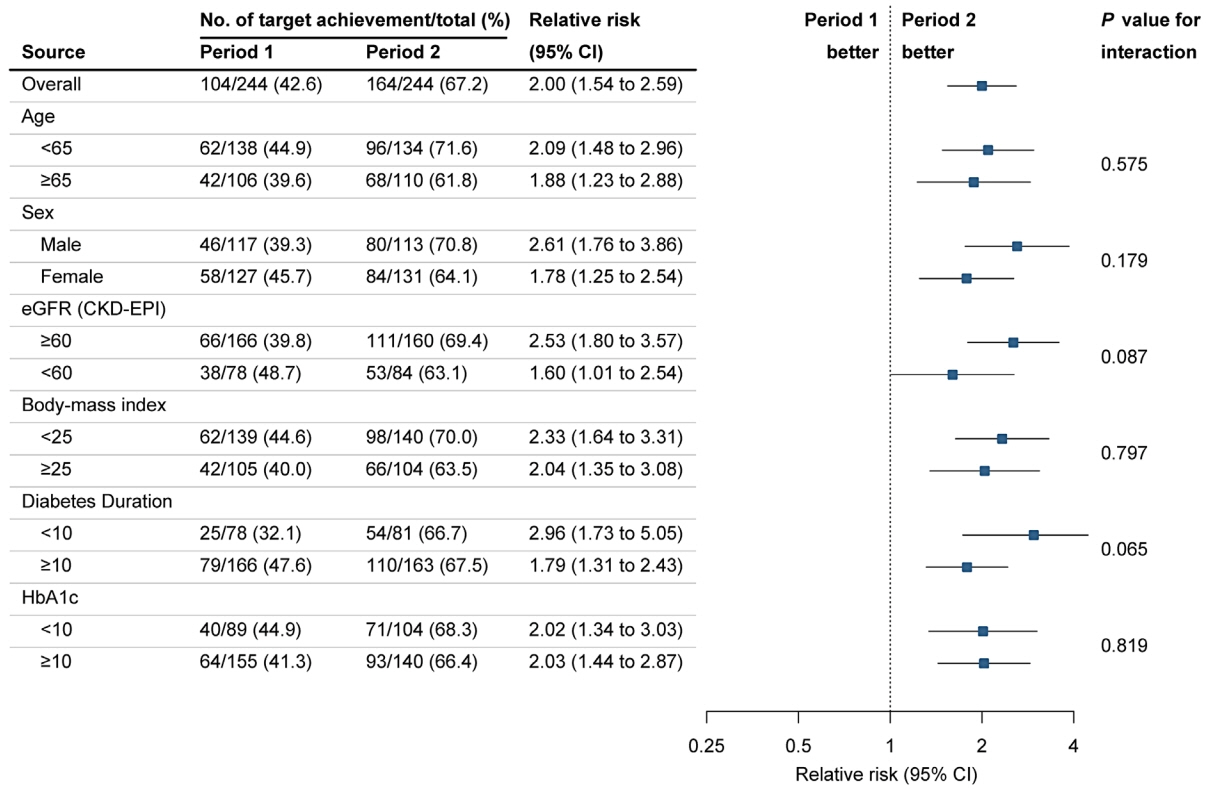
Fig. 2. Cox regression and subgroup analyses of the mean preprandial glycemic target achievement. Shown are the forest plots for patient subgroups with respect to the target glycemic achievements. Age, sex, body mass index, weight, estimated glomerular filtration rate (eGFR), diabetes duration, glycated hemoglobin (HbA1c), number of concurrent antidiabetic medications, the usage frequency of each antidiabetic medication, and the number of plasma glucose measurements by point-of-care testing were adjusted. P values describe the interaction between the target glycemic achievement and subgroup variables with no adjustment for multiple testing. CI, confidence interval; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration.
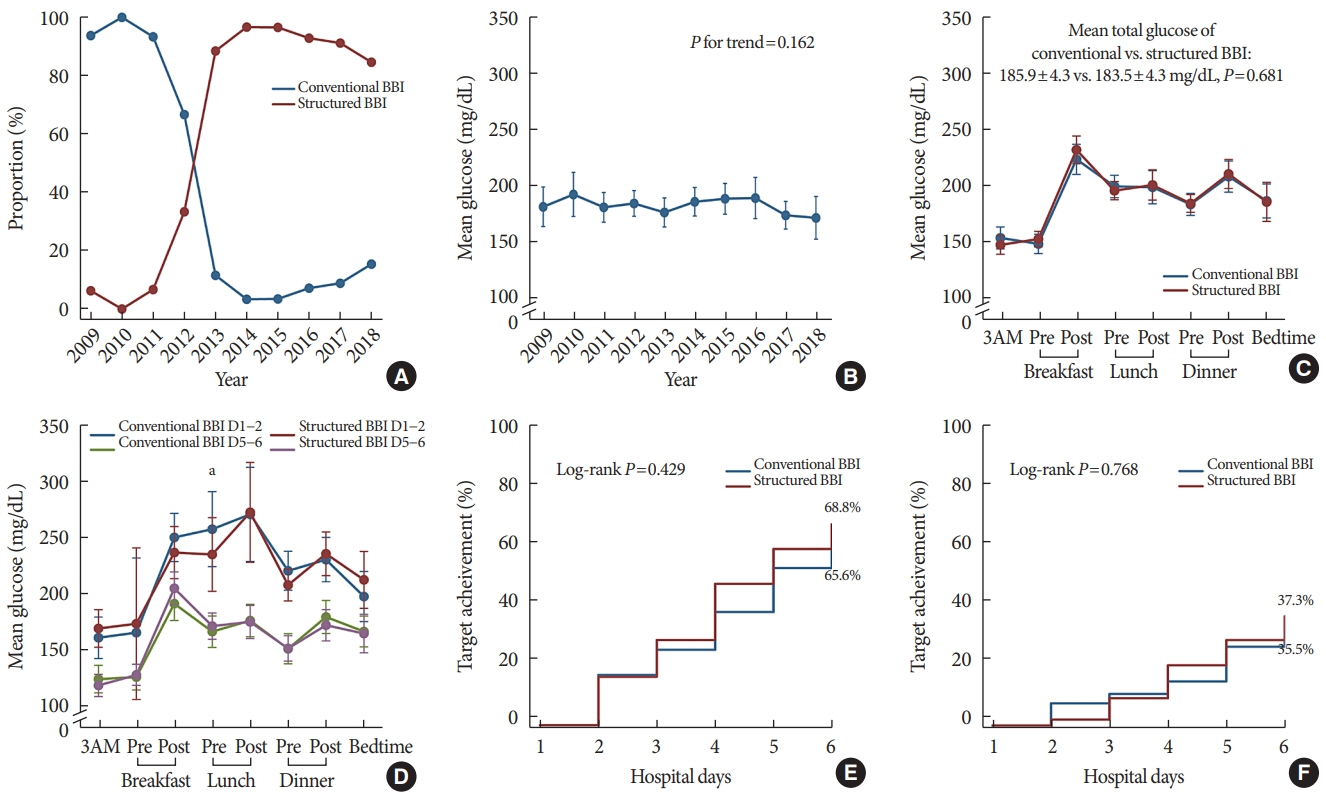
Fig. 3. Comparison of conventional vs. structured basal-bolus insulin (BBI). Data shown are the glucose values (estimated mean±standard error) obtained from each time point with 95% confidence intervals. Analysis of covariance (ANCOVA) analyses were performed, adjusted for age, sex, body mass index, weight, estimated glomerular filtration rate, diabetes duration, glycated hemoglobin, number of concurrent antidiabetic medications, the usage frequency of each antidiabetic medication, and the number of plasma glucose measurements by point-of-care testing. (A) Proportion of conventional and structured BBI from 2009 to 2018. (B) Mean glucose from 2009 to 2018. (C) Mean glucose from day 1 to 6 according to time of the day. (D) Mean glucose from day 1 to 2 vs. day 5 to 6. (E) Kaplan-Meier analysis of target achievement of the mean preprandial glucose on each day. (F) Kaplan-Meier analysis of target achievement of all preprandial glucose on each day.
Reference
-
1. International Diabetes Federation. IDF diabetes atlas. 9th ed. Brussels: IDF;2019. [cited 2021 Sep 25]. Available from: www.diabetesatlas.org/en.2. Cook CB, Kongable GL, Potter DJ, Abad VJ, Leija DE, Anderson M. Inpatient glucose control: a glycemic survey of 126 U.S. hospitals. J Hosp Med. 2009; 4:E7–14.
Article3. Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003; 78:1471–8.
Article4. Holman N, Knighton P, Kar P, O’Keefe J, Curley M, Weaver A, et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a population-based cohort study. Lancet Diabetes Endocrinol. 2020; 8:823–33.
Article5. van den Boom W, Schroeder RA, Manning MW, Setji TL, Fiestan GO, Dunson DB. Effect of A1C and glucose on postoperative mortality in noncardiac and cardiac surgeries. Diabetes Care. 2018; 41:782–8.
Article6. Umpierrez GE, Smiley D, Jacobs S, Peng L, Temponi A, Mulligan P, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care. 2011; 34:256–61.
Article7. Bagshaw SM, Egi M, George C, Bellomo R; Australia New Zealand Intensive Care Society Database Management Committee. Early blood glucose control and mortality in critically ill patients in Australia. Crit Care Med. 2009; 37:463–70.
Article8. Kosiborod M, Rathore SS, Inzucchi SE, Masoudi FA, Wang Y, Havranek EP, et al. Admission glucose and mortality in elderly patients hospitalized with acute myocardial infarction: implications for patients with and without recognized diabetes. Circulation. 2005; 111:3078–86.
Article9. Kosiborod M, Inzucchi SE, Krumholz HM, Xiao L, Jones PG, Fiske S, et al. Glucometrics in patients hospitalized with acute myocardial infarction: defining the optimal outcomes-based measure of risk. Circulation. 2008; 117:1018–27.
Article10. NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster D, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009; 360:1283–97.
Article11. Queale WS, Seidler AJ, Brancati FL. Glycemic control and sliding scale insulin use in medical inpatients with diabetes mellitus. Arch Intern Med. 1997; 157:545–52.
Article12. Browning LA, Dumo P. Sliding-scale insulin: an antiquated approach to glycemic control in hospitalized patients. Am J Health Syst Pharm. 2004; 61:1611–4.
Article13. Hirsch IB. Sliding scale insulin: time to stop sliding. JAMA. 2009; 301:213–4.14. Golightly LK, Jones MA, Hamamura DH, Stolpman NM, McDermott MT. Management of diabetes mellitus in hospitalized patients: efficiency and effectiveness of sliding-scale insulin therapy. Pharmacotherapy. 2006; 26:1421–32.
Article15. Umpierrez GE, Palacio A, Smiley D. Sliding scale insulin use: myth or insanity? Am J Med. 2007; 120:563–7.
Article16. Sheu WH, Ji L, Lee WJ, Jabbar A, Han JH, Lew T. Efficacy and safety of premixed insulin analogs in Asian patients with type 2 diabetes: a systematic review. J Diabetes Investig. 2017; 8:518–34.
Article17. Ji LN, Lu JM, Guo XH, Yang WY, Weng JP, Jia WP, et al. Glycemic control among patients in China with type 2 diabetes mellitus receiving oral drugs or injectables. BMC Public Health. 2013; 13:602.
Article18. Freemantle N, Balkau B, Danchin N, Wang E, Marre M, Vespasiani G, et al. Factors influencing initial choice of insulin therapy in a large international non-interventional study of people with type 2 diabetes. Diabetes Obes Metab. 2012; 14:901–9.
Article19. Roberts GW, Aguilar-Loza N, Esterman A, Burt MG, Stranks SN. Basal-bolus insulin versus sliding-scale insulin for inpatient glycaemic control: a clinical practice comparison. Med J Aust. 2012; 196:266–9.
Article20. Zaman Huri H, Permalu V, Vethakkan SR. Sliding-scale versus basal-bolus insulin in the management of severe or acute hyperglycemia in type 2 diabetes patients: a retrospective study. PLoS One. 2014; 9:e106505.
Article21. Cefalu WT, Dawes DE, Gavlak G, Goldman D, Herman WH, Van Nuys K, et al. Insulin Access and Affordability Working Group: conclusions and recommendations. Diabetes Care. 2018; 41:1299–311.
Article22. Hirao K, Arai K, Yamauchi M, Takagi H, Kobayashi M; Japan Diabetes Clinical Data Management Study Group. Six-month multicentric, open-label, randomized trial of twice-daily injections of biphasic insulin aspart 30 versus multiple daily injections of insulin aspart in Japanese type 2 diabetic patients (JDDM 11). Diabetes Res Clin Pract. 2008; 79:171–6.
Article23. Jeong IK, Chung CH, Zhou Z, Han JH, Duan R, Edralin DM, et al. Comparison of insulin intensification strategies with insulin lispro low mixture twice daily versus basal insulin glargine and prandial insulin lispro once daily in East Asian and Caucasian patients with type 2 diabetes mellitus. J Diabetes. 2017; 9:396–404.24. Ji L, Min KW, Oliveira J, Lew T, Duan R. Comparison of efficacy and safety of two starting insulin regimens in non-Asian, Asian Indian, and East Asian patients with type 2 diabetes: a post hoc analysis of the PARADIGM study. Diabetes Metab Syndr Obes. 2016; 9:243–9.25. Masuda H, Sakamoto M, Irie J, Kitaoka A, Shiono K, Inoue G, et al. Comparison of twice-daily injections of biphasic insulin lispro and basal-bolus therapy: glycaemic control and quality-of-life of insulin-naïve type 2 diabetic patients. Diabetes Obes Metab. 2008; 10:1261–5.
Article26. Jin SM, Kim JH, Min KW, Lee JH, Ahn KJ, Park JH, et al. Basalprandial versus premixed insulin in patients with type 2 diabetes requiring insulin intensification after basal insulin optimization: a 24-week randomized non-inferiority trial. J Diabetes. 2016; 8:405–13.
Article27. Jia W, Xiao X, Ji Q, Ahn KJ, Chuang LM, Bao Y, et al. Comparison of thrice-daily premixed insulin (insulin lispro premix) with basal-bolus (insulin glargine once-daily plus thrice-daily prandial insulin lispro) therapy in east Asian patients with type 2 diabetes insufficiently controlled with twice-daily premixed insulin: an open-label, randomised, controlled trial. Lancet Diabetes Endocrinol. 2015; 3:254–62.
Article28. Anyanwagu U, Mamza J, Gordon J, Donnelly R, Idris I. Premixed vs basal-bolus insulin regimen in Type 2 diabetes: comparison of clinical outcomes from randomized controlled trials and real-world data. Diabet Med. 2017; 34:1728–36.
Article29. Umpierrez GE, Smiley D, Zisman A, Prieto LM, Palacio A, Ceron M, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care. 2007; 30:2181–6.
Article30. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011; 10:150–61.
Article31. American Diabetes Association. 15. Diabetes care in the hospital: standards of medical care in diabetes-2021. Diabetes Care. 2021; 44(Suppl 1):S211–20.32. Bellido V, Suarez L, Rodriguez MG, Sanchez C, Dieguez M, Riestra M, et al. Comparison of basal-bolus and premixed insulin regimens in hospitalized patients with type 2 diabetes. Diabetes Care. 2015; 38:2211–6.
Article33. Alvarenga MA, Komatsu WR, de Sa JR, Chacra AR, Dib SA. Clinical inertia on insulin treatment intensification in type 2 diabetes mellitus patients of a tertiary public diabetes center with limited pharmacologic armamentarium from an upper-middle income country. Diabetol Metab Syndr. 2018; 10:77.
Article34. Lovshin JA, Zinman B. Diabetes: clinical inertia: a barrier to effective management of T2DM. Nat Rev Endocrinol. 2013; 9:635–6.
Article35. Blak BT, Smith HT, Hards M, Curtis BH, Ivanyi T. Optimization of insulin therapy in patients with type 2 diabetes mellitus: beyond basal insulin. Diabet Med. 2012; 29:e13–20.
Article36. Holt RI. Insulin initiation in type 2 diabetes: the implications of the 4-T study. Diabet Med. 2010; 27:1–3.
Article37. Liebl A. Insulin intensification: the rationale and the target. Int J Clin Pract Suppl. 2009; 164:1–5.38. Cho YM. To mix or to separate: that is the question. Lancet Diabetes Endocrinol. 2015; 3:229–31.
Article39. Kalra S, Balhara YP, Sahay BK, Ganapathy B, Das AK. Why is premixed insulin the preferred insulin?: novel answers to a decade-old question. J Assoc Physicians India. 2013; 61(1 Suppl):9–11.40. Wilson M, Weinreb J, Hoo GW. Intensive insulin therapy in critical care: a review of 12 protocols. Diabetes Care. 2007; 30:1005–11.41. Zhang X, Zhang T, Xiang G, Wang W, Li Y, Du T, et al. Comparison of weight-based insulin titration (WIT) and glucose-based insulin titration using basal-bolus algorithm in hospitalized patients with type 2 diabetes: a multicenter, randomized, clinical study. BMJ Open Diabetes Res Care. 2020; 8:e001261.
Article42. Wexler DJ, Shrader P, Burns SM, Cagliero E. Effectiveness of a computerized insulin order template in general medical inpatients with type 2 diabetes: a cluster randomized trial. Diabetes Care. 2010; 33:2181–3.43. Aloi J, Bode BW, Ullal J, Chidester P, McFarland RS, Bedingfield AE, et al. Comparison of an electronic glycemic management system versus provider-managed subcutaneous basal bolus insulin therapy in the hospital setting. J Diabetes Sci Technol. 2017; 11:12–6.
Article44. Li X, Du T, Li W, Zhang T, Liu H, Xiong Y. Efficacy and safety of weight-based insulin glargine dose titration regimen compared with glucose level- and current dose-based regimens in hospitalized patients with type 2 diabetes: a randomized, controlled study. Clin Ther. 2014; 36:1269–75.
Article45. Davis S, Friece C, Roderman N, Newcomer D, Castaneda E. Comparison of insulin detemir and insulin glargine for hospitalized patients on a basal-bolus protocol. Pharmacy (Basel). 2017; 5:22.
Article46. Lorenz E, Kopke S, Pfaff H, Blettner M. Cluster-randomized studies. Dtsch Arztebl Int. 2018; 115:163–8.
Article47. Campbell MK, Mollison J, Steen N, Grimshaw JM, Eccles M. Analysis of cluster randomized trials in primary care: a practical approach. Fam Pract. 2000; 17:192–6.
Article48. Wang C, Mamza J, Idris I. Biphasic vs basal bolus insulin regimen in type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabet Med. 2015; 32:585–94.49. Perez A, Reales P, Barahona MJ, Romero MG, Minambres I; HOSMIDIA Study Group. Efficacy and feasibility of basal-bolus insulin regimens and a discharge-strategy in hospitalised patients with type 2 diabetes: the HOSMIDIA study. Int J Clin Pract. 2014; 68:1264–71.50. Akhtar ST, Mahmood K, Naqvi IH, Vaswani AS. Inpatient management of type 2 diabetes mellitus: does choice of insulin regimen really matter? Pak J Med Sci. 2014; 30:895–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Insulin Treatment in Hospitalized Patients
- Real-World Analysis of Therapeutic Outcome in Type 1 Diabetes Mellitus at a Tertiary Care Center
- Intraoperative and Postoperative Glycemic Management in Patients with Diabetes
- Real-World Efficacy and Safety of Dulaglutide in Korean Patients with Type 2 Diabetes Mellitus: A Retrospective Study in a Tertiary Referral Center
- The Changes in the Outbreak of Rotavirus Gastroenteritis in Children after Introduction of Rotavirus Vaccines: A Retrospective Study at a Tertiary Hospital
