Metastatic ameloblastoma with postoperative accelerated tumor growth treated with carboplatin and paclitaxel: a case report
- Affiliations
-
- 1Division of Pulmonary Medicine, Department of Internal Medicine, Wonkwang University Hospital, Iksan, Korea
- KMID: 2527699
- DOI: http://doi.org/10.7180/kmj.21.030
Abstract
- Ameloblastoma is a histologically benign odontogenic epithelial tumor that rarely metastasizes. However, metastasis to the lungs can occur, usually years after the development of the primary tumor. Here, we present the case of a 63-year-old woman with metastatic ameloblastoma in the lungs that developed 12 years after surgery for the primary lesion. As is typical for metastatic ameloblastomas, the tumor was incidentally found on radiography and surgically removed. However, the tumor exhibited accelerated progression with pleural metastasis after surgical removal, which is unusual in metastatic ameloblastoma. The patient was successfully treated with carboplatin/paclitaxel and showed a partial response to tumor progression, implying that this approach can be safely used in the absence of a standard treatment regimen.
Keyword
Figure
-

Fig. 1. Initial chest computed tomography performed in October 2013. (A) A 13-mm heterogeneous enhancing solid nodule with a peripheral ground-glass opacity in the right lower lobe (arrow). (B) An 8-mm small, noncalcified nodule in the right middle lobe (arrow).
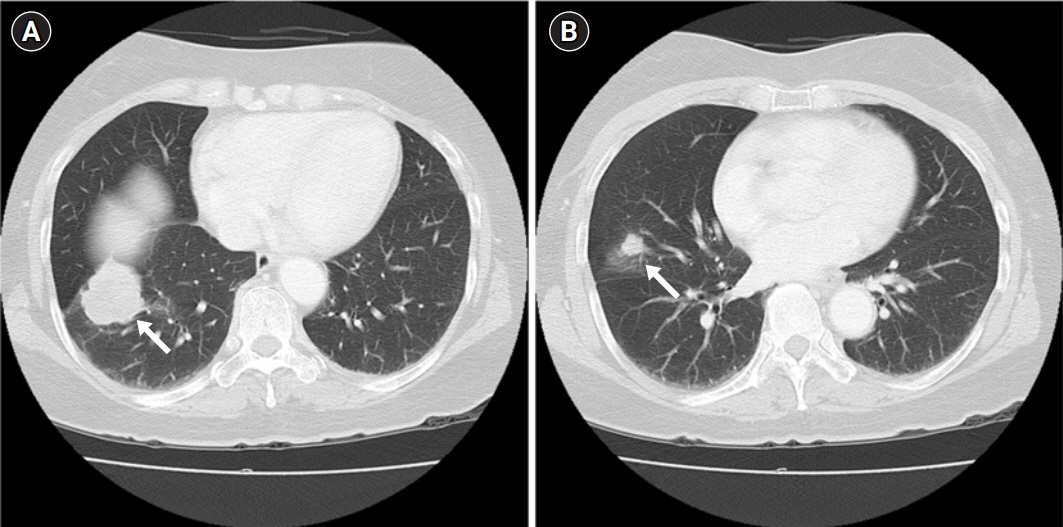
Fig. 2. Follow-up chest computed tomography performed in March 2020. (A) A 45-mm well-defined, lobulated, heterogeneously enhancing mass with a peripheral ground-glass opacity, abutting the right major fissure and diaphragm and causing pleural retraction in the right lower lobe (arrow). (B) A 14-mm, spiculated-margin, enhancing solid nodule with pleural retraction in the right middle lobe (arrow).

Fig. 3. Pathological findings of the lung biopsy specimen. (A) The pulmonary metastatic lesion is more cellular, with a clear margin between the lesion and the surrounding lung tissue (H&E, ×40). (B) Anastomosing epithelial strands show peripheral palisading (arrows) with more loosely arranged angular cells (arrowheads) and variable keratinization (asterisk) (H&E, ×100). (C) CD56 is preferentially expressed in peripheral cells, and (D) CK19 is expressed in all cells (immunohistochemical stain, ×100).
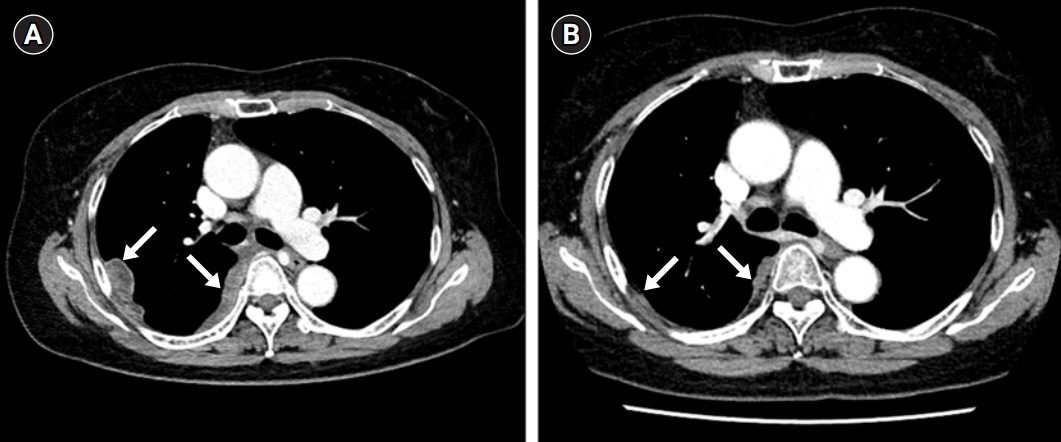
Fig. 4. (A) Chest computed tomography performed in July 2020. Newly developed multifocal enhancing pleural and fissural nodules in the right hemithorax (arrows). (B) Follow-up chest computed tomography performed after chemotherapy, showing markedly decreased size of the previously noted pleural and fissural nodules in the right hemithorax (arrows).
Reference
-
References
1. Ghiam A, Al Zahrani A, Feld R. A case of recurrent metastatic ameloblastoma and hypercalcaemia successfully treated with carboplatin and paclitaxel: long survival and prolonged stable disease. Ecancermedicalscience. 2013; 7:323.2. Li D, Xu S, Sun M, Qiao L, Wang L, Liu Y. MAID chemotherapy regimen as a treatment strategy for metastatic malignant ameloblastoma: a case report. Medicine (Baltimore). 2019; 98:e15873.3. Mendenhall WM, Werning JW, Fernandes R, Malyapa RS, Mendenhall NP. Ameloblastoma. Am J Clin Oncol. 2007; 30:645–8.
Article4. Valkadinov I, Conev N, Dzhenkov D, Donev I. Rare case of ameloblastoma with pulmonary metastases. Intractable Rare Dis Res. 2017; 6:211–4.
Article5. Amzerin M, Fadoukhair Z, Belbaraka R, Iraqui M, Boutayeb S, M'rabti H, et al. Metastatic ameloblastoma responding to combination chemotherapy: case report and review of the literature. J Med Case Rep. 2011; 5:491.
Article6. Van Dam SD, Unni KK, Keller EE. Metastasizing (malignant) ameloblastoma: review of a unique histopathologic entity and report of Mayo Clinic experience. J Oral Maxillofac Surg. 2010; 68:2962–74.
Article7. Inoue N, Shimojyo M, Iwai H, Ohtsuki H, Yasumizu R, Shintaku M, et al. Malignant ameloblastoma with pulmonary metastasis and hypercalcemia. Report of an autopsy case and review of the literature. Am J Clin Pathol. 1988; 90:474–81.
Article8. Wright JM, Vered M. Update from the 4th edition of the World Health Organization Classification of Head and Neck Tumours: odontogenic and maxillofacial bone tumors. Head Neck Pathol. 2017; 11:68–77.
Article9. Senra GS, Pereira AC, Murilo dos Santos L, Carvalho YR, Brandao AA. Malignant ameloblastoma metastasis to the lung: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:e42–6.
Article10. Tohme S, Simmons RL, Tsung A. Surgery for cancer: a trigger for metastases. Cancer Res. 2017; 77:1548–52.
Article11. Murthy SM, Goldschmidt RA, Rao LN, Ammirati M, Buchmann T, Scanlon EF. The influence of surgical trauma on experimental metastasis. Cancer. 1989; 64:2035–44.
Article12. Ciment LM, Ciment AJ. Malignant ameloblastoma metastatic to the lungs 29 years after primary resection: a case report. Chest. 2002; 121:1359–61.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of neoadjuvant chemotherapy with taxol / carboplatin in advanced epithelial ovarian cancer
- Quantitative analysis of proteins related to chemoresistance to paclitaxel and carboplatin in human SiHa cervical cancer cells via iTRAQ
- A Case of Recurrent Cervical Cancer Responded to Paclitaxel and Carboplatin Combination
- Postoperative Radiation Therapy in Ameloblastoma of the Jaw: Report of Two Cases
- Metastatic Cervical Lymphadenopathy from Uterine Leiomyosarcoma with Good Local Response to Radiotherapy and Chemotherapy
